

Atrial pacing
There are a number of manufacturer-specific features in terms of automatic atrial threshold measurement and automatic programming adaptation.
- Biotronik, Boston Scientific, Medtronic and Abbott pacemakers enable automatic measurement of atrial pacing threshold, with adaptation of programming; Microport CRM-Sorin pacemakers do not.
- The various systems do not work with cycle-by-cycle capture verification; threshold is measured every X hours (variable depending on the manufacturer) with programming adaptation for the period between 2 threshold measurements.
- Threshold measurement is based on spontaneous atria or ventricles for Biotronik and Medtronic pacemakers, on evoked response for Boston Scientific pacemakers and on morphology for Abbott pacemakers.
Contents
Abbott
Operating principles
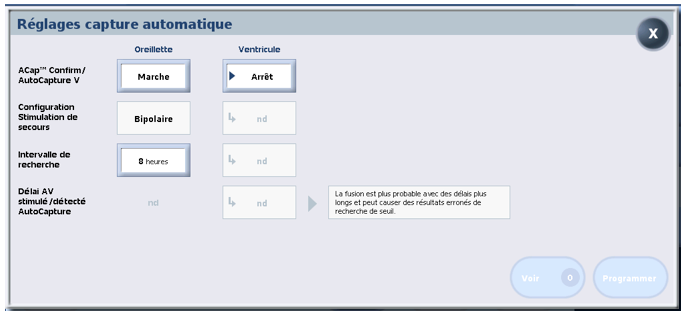
- ACap Confirm ON: the atrial stimulation threshold is measured and stored automatically on the curve + automatic adaptation of programming; ACap Confirm on monitor: the atrial stimulation threshold is measured and stored automatically without automatic adaptation of programming
- threshold performed systematically every 8 or 24 hours, depending on the setting of the Search interval parameter
- capture control based on analysis of the morphology of the atrial evoked response
- no cycle-by-cycle control of capture and adaptation for every 8 hours
- variable safety margin depending on threshold: if threshold ≤ 1. 5V, margin at + 1.0V; if threshold between 1.625V and 2.25V, margin at + 1.5V; if threshold between 2.375V and 3.0V, margin at + 2.0V; if threshold > 3V, amplitude at 5V
- maximum amplitude that can be delivered: 5 V for programmed pulse duration
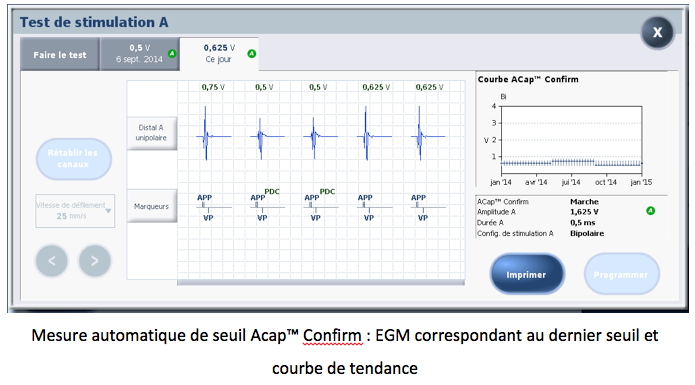
ACap Confirm in practice
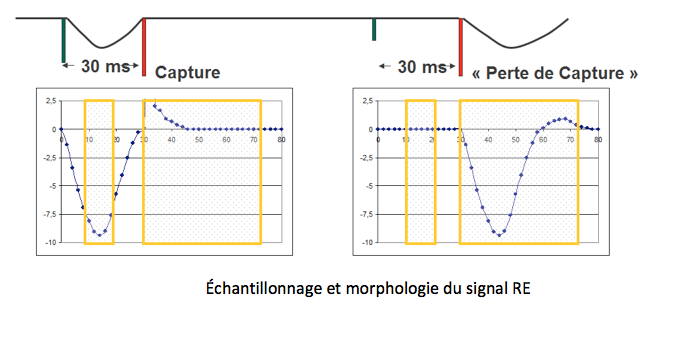
Atrial threshold control is based on analysis of the morphology of the atrial evoked response, but without cycle-by-cycle monitoring and verification of capture. The device memorizes the morphology of the failed capture. The morphology is made up of measurement points sampled between the first stimulus and the backup stimulus at 5 V (30 ms after the first) and measurement points following the backup stimulus. The capture loss model is updated before each threshold measurement during the configuration test.
During the configuration test, an essential prerequisite for threshold measurement, 3 pairs of stimuli are delivered to test the morphology of the evoked response (ER):
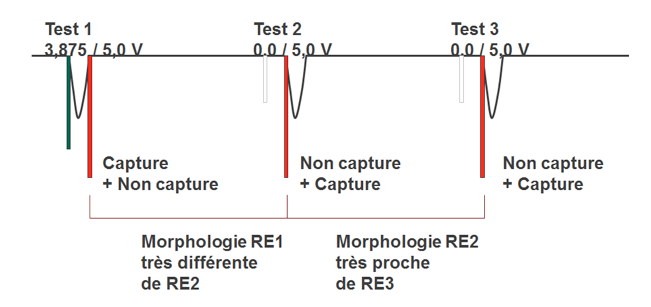
Acap Confirm uses a score to differentiate between loss-of-capture and capture morphologies. If the capture score is significantly different from the loss-of-capture score, then the configuration is recommended and the stimulation threshold is automatically measured.
Tests 2 and 3 are used to update the capture loss model. The RE morphology loss-of-capture model is continuously updated.
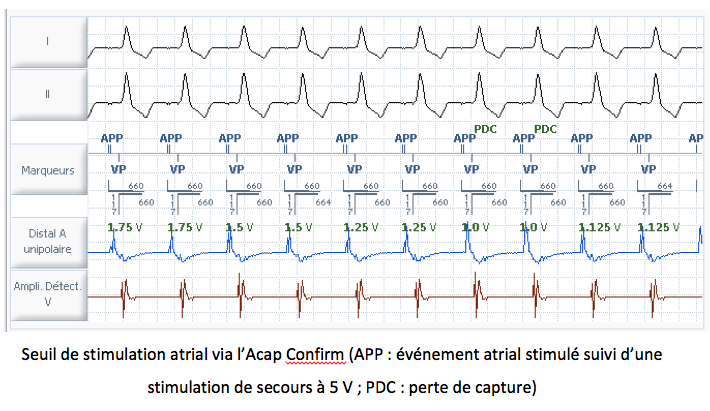
The 5 V backup stimulus is delivered cycle by cycle during the threshold, whether the first stimulus is captured or fails to be captured, so that the morphology score can be assessed.
Following a threshold measurement every 8 or 24 hours, the atrial amplitude is automatically adapted with the following margin:
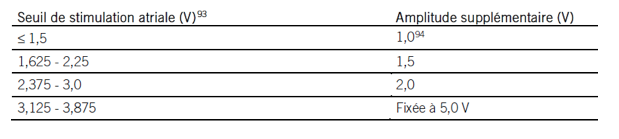
If the stimulation threshold determined by the algorithm exceeds 3.875 V, Acap Confirm is automatically deactivated and the pulse amplitude is reprogrammed to 5 V.
Biotronik
Operating principles
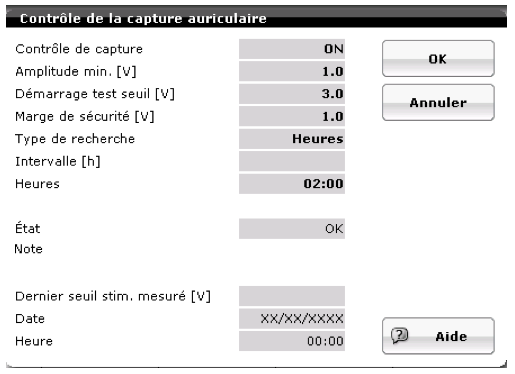
- atrial capture control ON: automatic measurement of atrial stimulation threshold + adaptation of programming; atrial capture control on ATM: automatic measurement of atrial stimulation threshold without adaptation; atrial capture control on stop: no automatic threshold measurement
- atrial stimulation threshold performed systematically every day at 2:00 a.m. (or programmable according to intervals: 24h, 12h, 6h, 3h, 1h, 0.3h, 0. 1h)
- atrial stimulation threshold based on detected atrial signals indicative of loss of capture
- no cycle-by-cycle verification of capture; amplitude adaptation for the following 24 hours
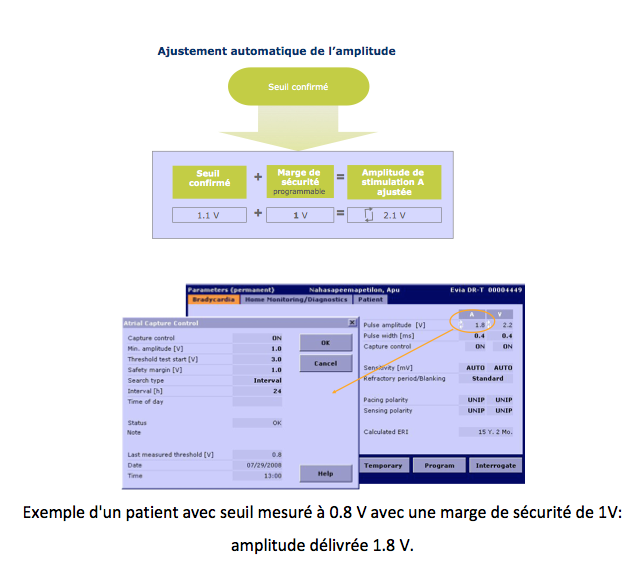
- programmable safety margin (nominal value + 1 V)
- maximum amplitude that can be delivered: test start amplitude i.e. 4.8V V for 0.4 ms
- minimum amplitude that can be delivered programmable: nominal value 1 V
Automatic control of atrial capture in practice
There are many similarities with ventricular capture control, but also some differences. Automatic atrial capture control is not based on evoked response analysis, but on the detection of atrial signals indicative of loss of capture: resumption of intrinsic rhythm or retrograde conduction if the patient is atrial dependent (sinus dysfunction).
The programmable parameters are the same (on, off and ATM options), but some nominal values are different: minimum amplitude is programmable with a nominal value of 1 V; safety margin, nominal value of 1 V;
For threshold measurement, the atrial pacing rate is increased to exceed the spontaneous atrial rate. If the spontaneous frequency is below 108 bpm, the threshold is performed at a frequency 20% higher than the spontaneous frequency. If the spontaneous rate is higher than 108 bpm, the test cannot be performed.
The test is performed in DDI mode with an AV delay of 50 ms and a post ventricular stimulation atrial blanking of 150 ms.
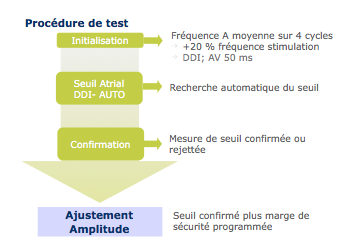
As with ventricular control, the threshold procedure starts at the programmed value and is reduced in 0.6 V steps until 2 out of 5 spontaneous atrial cycles are detected. The second phase of 0.1 V steps is identical to that of ventricular control.
Each amplitude is tested 5 times in succession.
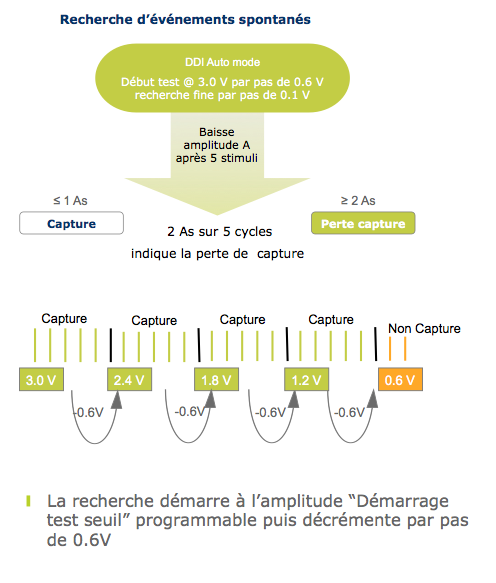
Synchronization atrial pacing (restoration of normal atrio-ventricular synchronization to prevent PMT) is delivered at the end of each series of 5 stimuli. The amplitude of this atrial stimulation varies according to the pitch (0.1 or 0.6 V) and the existence of a capture.
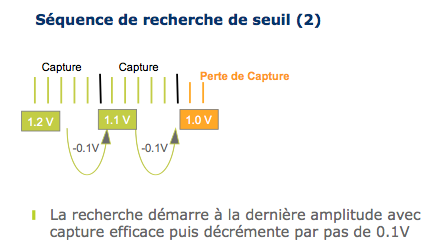
The measured threshold is then confirmed in 2 steps: a stimulation amplitude 0.3 V above the measured threshold is repeated 5 times (step 1), then a stimulation amplitude 0.3 V below the measured threshold is repeated 2 times (step 2). 2 out of 5 capture losses are sufficient, followed by a safety stimulation. Threshold is confirmed if capture is present during step 1 and absent during step 2.
The stimulation amplitude is adapted by adding the value of the safety margin.
Boston Scientific
Operating principles
- Atrial amplitude on AUTO: measurement of the atrial stimulation threshold + adaptation of the programming; atrial amplitude on fixed value and Daily trends on ON: measurement of the atrial stimulation threshold without adaptation
- threshold systematically performed every 21 hours
- threshold measurement based on analysis of the atrial evoked response (OD ring – box)
- no cycle-by-cycle control of capture but adaptation for every 21 hours
- non-programmable safety margin of 2 times the measured threshold
- maximum amplitude that can be delivered: 5 V for 0. 4 ms
- minimum deliverable amplitude: 2 V for 0.4 ms
The PaceSafe OD algorithm in practice
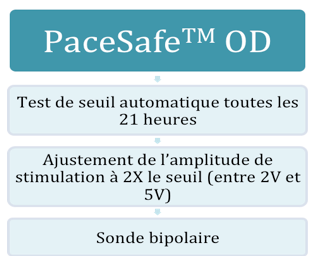
This algorithm can only work if the atrial lead is bipolar. It is activated by setting the atrial pacing amplitude to AUTO. The atrial pacing threshold is measured every 21 hours and the pacing amplitude adapted for the next 21 hours. The safety margin corresponds to twice the measured threshold, as the amplitude delivered cannot be less than 2 V or greater than 5 V. The safety margin can therefore only be double the threshold if the threshold is less than 2.5 V. Pulse duration is set at 0.4 ms. The threshold is unipolar. This algorithm only works if the threshold is between 0.2 and 4 V.
Assessment of atrial capture is based on evoked response analysis. The starting atrial stimulation amplitude corresponds to the amplitude delivered at the time of testing. The stimulated AV delay is set at 85 ms, the detected AV delay at 55 ms. The pacing frequency is set to the mean atrial frequency, the minimum frequency or the frequency indicated by the sensor, whichever is faster. If the number of atrial stimulations is insufficient, the atrial stimulation frequency is increased by 10 bpm.
Following initialization pacing, the pacemaker decreases atrial pacing amplitude every 3 beats until loss of capture (determined by the absence of an atrial evoked response) and threshold determination. If a loss of capture occurs 2 times during the 3 measurements, the threshold is defined as the previous value tested. To avoid the occurrence of an PMT, the PVARP is lengthened to 500 ms following a loss of atrial capture.
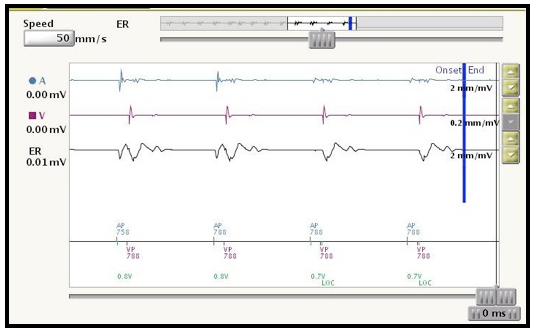
Example of an atrial threshold test with capture at 0.8 V (presence of atrial evoked response) and loss of capture at 0.7 V (LOC, loss of capture, absence of atrial evoked response).
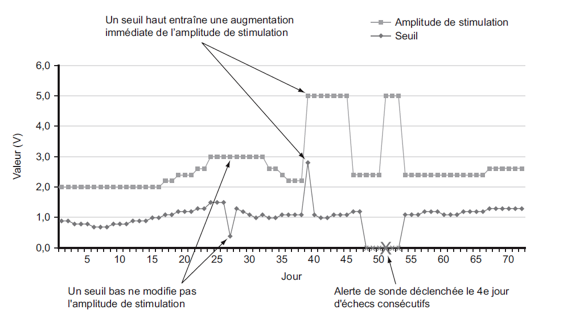
Pacing amplitude is not adjusted to correspond to 2 times the last measured threshold value, but to correspond to the maximum threshold measured during the last 7 ambulatory tests. This allows a rapid increase in amplitude if a sudden increase in threshold is observed. On the other hand, a single low threshold value does not reduce the stimulation amplitude.
There is therefore no cycle-to-cycle adaptation or backup stimulation.
Medtronic
Operating principles
- dynamic atrial threshold control: daily measurement of atrial stimulation threshold + programming adaptation for 24 hours; monitor-based atrial capture control: measurement of atrial stimulation threshold without adaptation; atrial threshold control on stop: fixed values and no automatic threshold measured
- threshold systematically measured every 24 hours at 1:00 a.m. atrial threshold measurement based on synchronization of detected P and R waves (2 methods depending on presence or absence of atrioventricular conduction)
- a single daily measurement with adaptation for the following 24 hours
- target amplitude by multiplying the OD amplitude safety margin by the threshold measured at a pulse duration of 0, 4 ms within an output range defined by a programmable lower limit (parameter Adjusted minimum amplitude) and the upper threshold limit of 5.0 V and 1.0 ms. The minimum pulse duration for atrial threshold control is 0.4 ms.
- maximum deliverable amplitude: 5 V for 1 ms
- minimum deliverable amplitude: 1 V for 0.4 ms
Atrial capture management (ACM) in practice
ACM is available when the device is operating in DDD(R) and MVP modes (AAI(R)<=>DDD(R)). If the stimulation mode programmed is MVP mode, the device temporarily switches to DDD(R) mode for the duration of the stimulation threshold search.
Before initiating a pacing threshold search, the stimulator assesses whether the patient is being paced, or whether there is a detection at a slow frequency. An atrial pacing threshold search is performed when a stable atrial rhythm is observed for eight pacing cycles and the sensor frequency is below the AQ frequency.
Atrial capture management (ACM) observes the synchronization of detected P and R waves (not an evoked response) to assess the degree of entrainment.
ACM automatically selects one of two methods to assess atrial entrainment, depending on the patient’s rhythm at the time of the pacing threshold search.
If the patient’s sinus rhythm is normal and stable, the device selects the atrial cavity reset (ACR) method. Otherwise, the device selects the AV conduction method (AVC).
Atrial cavity reset (ACR) is used to assess entrainment by observing the intrinsic rhythm response to test atrial pacing. If test pacing does not entrain, the sinus node is not reset and an atrial event detected in the refractory period is observed after test pacing. If no refractory-period atrial event is observed during the AV delay, ACR concludes that test pacing has entrained the myocardium.
The AV conduction method (AVC) is performed when stable 1:1 AV conduction is observed during atrial pacing. The atrial pacing rate is increased by 15 bpm (but not more than 101 bpm) and the AV delay is lengthened in an attempt to achieve a stable AP-VS rhythm. The AVC assesses the degree of entrainment by observing the ventricular response to test atrial pacing. Each test atrial pacing event is followed by a backup pacing event at a programmed amplitude and pulse duration of 1.0 ms to ensure that the rhythm remains stable throughout the test. If a ventricular lead sensing event is observed at the predicted AP-VS interval (approximately) following test atrial pacing, the AVC concludes that test pacing has entrained the myocardium.
A stimulation threshold search starts at an amplitude 0.125 V below the last measured threshold. In the absence of a previous search, a new search begins at 0.75 V. The device continues to decrease amplitude in steps of 0.125 V until capture is lost. It then increases the test amplitude in steps of 0.125 V until capture is achieved 3 times in succession. This amplitude corresponds to the atrial stimulation threshold.
The target amplitude is based on the values programmed for the parameters A. amplitude safety margin and Minimum adjusted atrial amplitude.
Atrial threshold control does not define atrial output at values above 5.0 V or 1.0 ms. Atrial amplitude and pulse duration must be programmed manually if the patient requires an atrial pacing output greater than 5.0 V or 1.0 ms.
Microport
Microport pacemakers do not automatically measure atrial threshold.