Abbott - Pacing / Detection
Atrial pacing
Operating principles
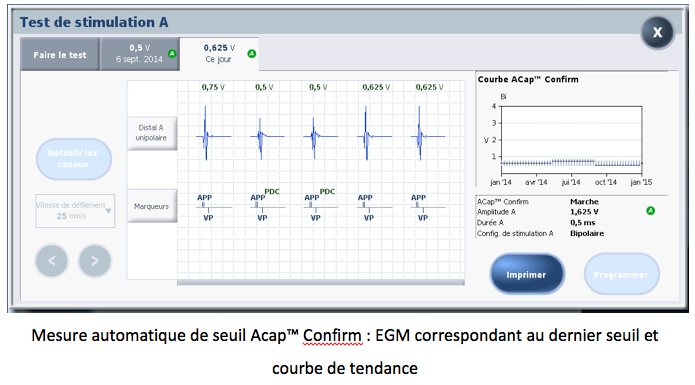
- ACap Confirm activated: the atrial pacing threshold is measured and stored automatically on the curve + automatic programming adaptation;
- ACap Confirm on monitor: the atrial pacing threshold is measured and stored automatically without automatic programming adaptation
- threshold measured systematically every 8 or 24 hours, depending on the Search Interval parameter setting
- capture control based on analysis of the morphology of the atrial evoked response
- no cycle-to-cycle capture control and adaptation for 8 hours
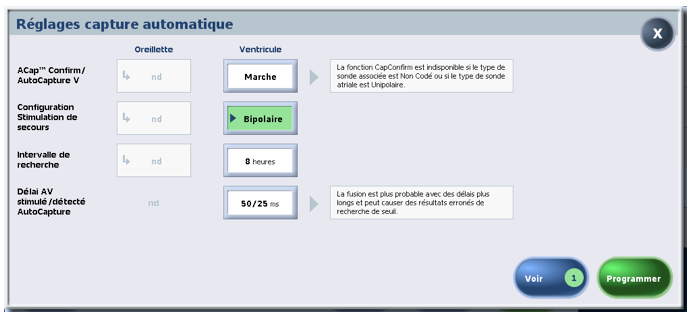
- safety margin variable depending on the threshold: if threshold ≤ 1.5V, margin at + 1.0V; if threshold between 1.625V and 2.25V, margin at + 1.5V; if threshold between 2.375V and 3.0V, margin at + 2.0V; if threshold > 3V, amplitude at 5V
- maximum amplitude that can be delivered: 5 V for programmed pulse duration
Acap Confirm in practice
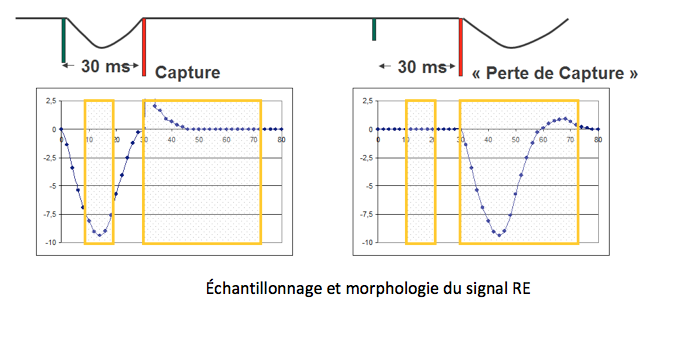
Atrial threshold control is based on analysis of the morphology of the atrial evoked response, but without cycle-by-cycle monitoring and verification of capture. The device stores the morphology of the capture failure. The morphology consists of measurement points sampled between the first stimulus and the 5 V back-up stimulus (30 ms after the first) and measurement points following the back-up stimulus. The capture loss model is updated before each threshold measurement during the configuration test.
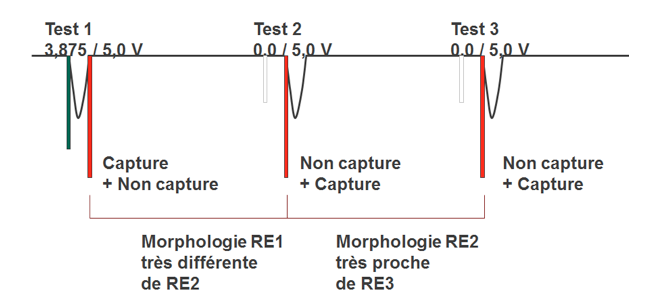
During the configuration test, which is an essential prerequisite for threshold measurement, three pairs of stimuli are delivered to test the morphology of the evoked response (ER):
Acap Confirm uses a score to differentiate between capture loss morphology and capture morphology. If the capture score is very different from the capture loss score, then the configuration is recommended and the stimulation threshold is automatically measured.
Tests 2 and 3 are used to update the loss-of-capture model. The ER morphology model for loss of capture is continuously updated.
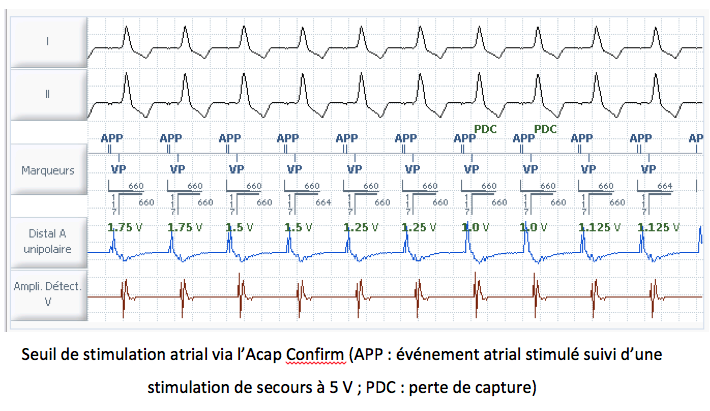
The 5 V back-up stimulus is delivered cycle by cycle during the threshold, regardless of whether the first stimulus is captured or fails to be captured, in order to evaluate the morphology score.
Following a threshold measurement taken every 8 or 24 hours, the atrial amplitude is automatically adjusted with the following margin:
If the stimulation threshold determined by the algorithm exceeds 3.875 V, Acap Confirm is automatically deactivated and the pulse amplitude is reprogrammed to 5 V.
Ventricular pacing
Operating principles
- Ventricular AutoCapture on: measurement of ventricular pacing threshold + programming adaptation with cycle-by-cycle monitoring;
- threshold measured systematically at least every eight hours (alternative programming option: measurement every 24 hours)
- cycle-by-cycle monitoring of capture based on analysis of evoked response
- safety margin of 0.25 V
- maximum amplitude that can be delivered: 4.5 V for programmed pulse duration
Ventricular AutoCapture in practice
The ventricular AutoCapture pacing system automatically adjusts the ventricular pulse amplitude of the pacemaker above the patient threshold measured regularly (at least every eight hours) and allows cycle-by-cycle capture verification. To use the AutoCapture V function in Microny or Victory pacemakers (and previous series), it was necessary to implant a bipolar ventricular lead. The detection mode had to be programmed as bipolar and the pacing mode as unipolar.
Since the Zephyr pacemaker platform (and subsequent ranges: Accent, Endurity, Assurity), AutoCapture can be activated regardless of the programmed detection and pacing configurations: Uni pacing/Uni detection; Bi pacing/Bi detection; Bi pacing/Uni detection; Uni pacing/Bi detection.
An automatic configuration test, used to check the compatibility of the probe based on its polarization and to differentiate between capture and capture failure, precedes the first activation request. This test remains optional (but recommended) before each threshold measurement.
Three AutoCapture V parameter settings are available:
- Configuration: this setting is available during the first activation. The programmer then proposes to start the Configuration Test and then the Stimulation Test if AutoCapture is recommended;
- On: the device measures the threshold, automatically adjusts the pulse amplitude, records the threshold measurement in the Threshold Curve, and stores the EGM corresponding to the last threshold;
- Off: the device does not measure the stimulation threshold and does not automatically adjust the pulse amplitude.
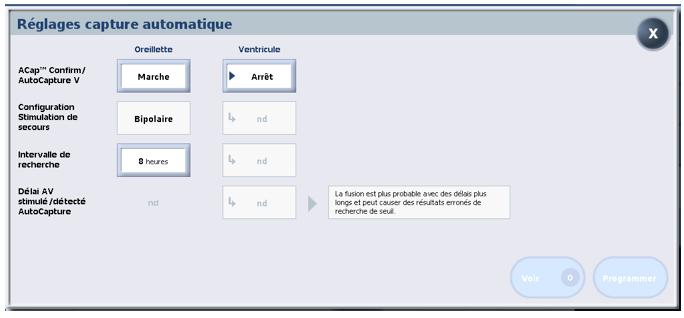
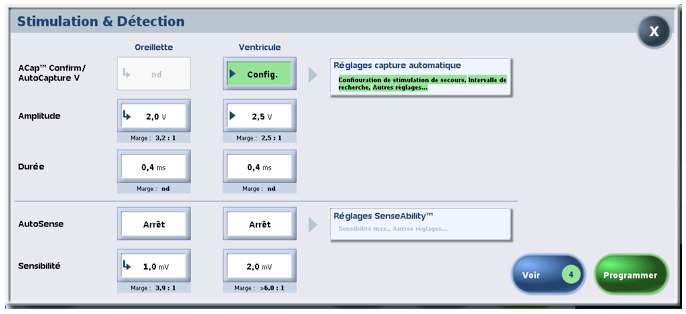
The following parameters can be adjusted in the AutoCapture Settings window:
- the backup pacing configuration, which allows you to program the polarity configuration of the backup pacing to bipolar or unipolar (default value);
- the search interval, which programs the frequency of threshold measurement to 8 hours (default value) or 24 hours;
- the stimulated/detected AV delays for AutoCapture™ V, which program the stimulated AV delay and detected AV delay parameters used during a threshold search to 50/25 ms (nominal value), 100/70 ms, or 120/100 ms. The recommended setting for this parameter is 50/25 to avoid mergers. Mergers are more likely with longer delays and can result in incorrect threshold search results.
The AutoCaptureTM system uses four algorithms to monitor capture cycle by cycle:
- capture verification
- capture loss recovery
- fusion avoidance
- periodic measurement of the stimulation threshold
1 – Capture verification
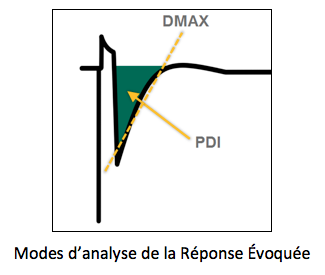
Verification of capture effectiveness is based on an analysis of the Evoked Response (ER). If the ventricular pacing configuration is programmed to bipolar, the area under the curve is used (Paced Depolarization Integral). If the ventricular pacing configuration is programmed to unipolar, the signal slope (DMAX) is used.
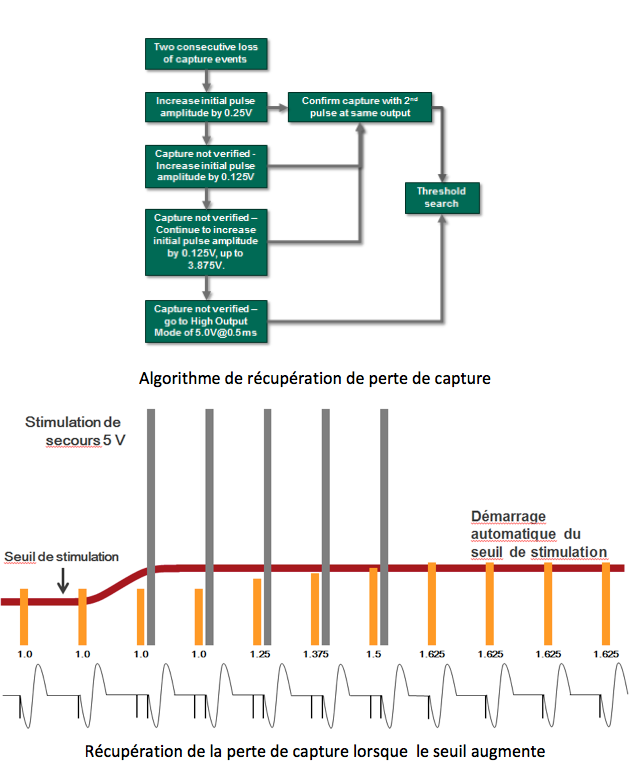
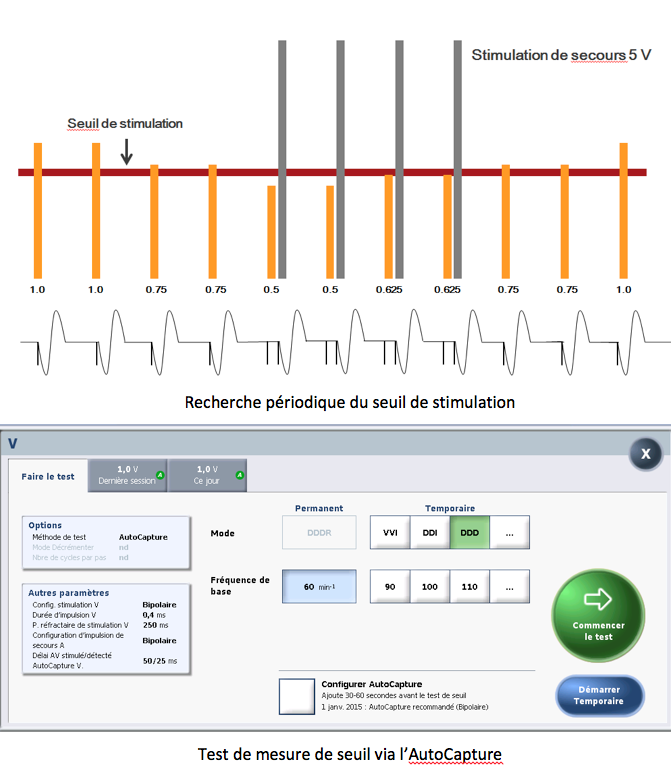
Mesure périodique du seuil de stimulation
- Lorsque la recherche automatique du seuil est amorcée (toutes les 8h ou 24h), l’appareil diminue l’amplitude d’impulsion de 0,25 V tous les deux cycles
- Si cela conduit à une perte de capture, l’appareil émet une impulsion de secours de 5 V (marge de sécurité), 80 à 100 ms après la première impulsion test
- En cas de perte de capture sur deux cycles consécutifs à la même amplitude, l’algorithme augmente alors l’amplitude d’impulsion par pas de 0,125 V tous les deux cycles
- Deux captures consécutives à la même amplitude doivent être confirmées pour déterminer la nouvelle valeur du seuil de stimulation
- Lorsque celle-ci est trouvée, l’appareil détermine une nouvelle Amplitude automatique en ajoutant une marge de travail de 0,25 V
- Si la recherche décroissante ne parvient pas à déterminer une perte de capture au plus faible réglage d’amplitude d’impulsion, c’est-à-dire 0 V, l’appareil commute sur « Mode haute amplitude » pour une durée de 128 cycles cardiaques, puis relance la recherche du seuil
- Si le seuil de stimulation déterminé par l’algorithme dépasse 3,875 V pour une certaine durée d’impulsion, l’AutoCapture est désactivé automatiquement et l’amplitude d’impulsion est reprogrammée à 5 V (Mode haute amplitude) ; un réglage plus élevé de la durée d’impulsion peut
permettre dans ce cas la réactivation de l’AutoCapture
La recherche du seuil est répétée:
- Après chaque opération de récupération de perte de capture
- Automatiquement toutes les 8 heures (ou 24 heures)
- Au retrait de la tête de télémétrie
- Au retrait de l’aimant
- Lorsque l’opérateur exécute le test de seuil de stimulateur via l’Autocapture
 Vérification de la capture
Vérification de la capture
La vérification de l’efficacité de la capture repose sur une analyse de la Réponse Évoquée
(RE).
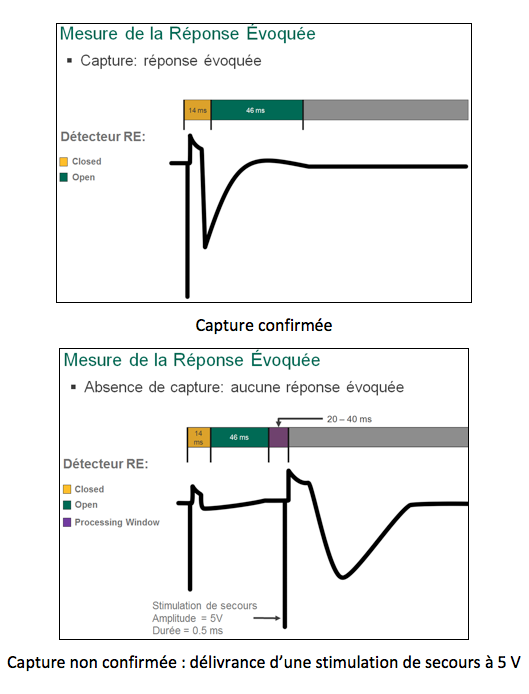
- Pour vérifier l’efficacité de la capture ventriculaire, il existe une première phase de blanking de 14 ms après la stimulation ventriculaire puis une fenêtre de recherche de la réponse évoquée de 46 ms
- Si l’appareil détecte une réponse évoquée dans cette fenêtre, la capture est confirmée
- Si aucun signal de réponse évoquée n’est détecté, l’appareil émet une impulsion de secours de 5 V dans les 80 à 100 ms suivant l’impulsion initiale afin d’assurer une capture
To verify the existence of the capture, there is an initial blanking phase of 14 ms followed by a 46 ms window for searching for the evoked response. If the device detects an evoked response within this window, the capture is confirmed. If no evoked response signal is detected, the device emits a 5 V backup pulse within 80 to 100 ms of the initial pulse to ensure capture.
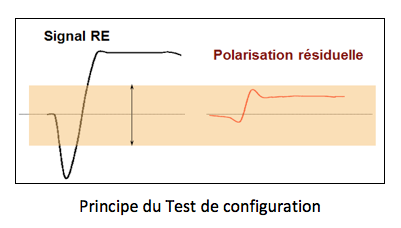
A configuration test is required to confirm that the AutoCapture system is working with the implanted probe. This test measures the evoked response and polarization artifact to enable effective capture assessment. It is used to determine an appropriate ER detection sensitivity. If there is sufficient margin between the ER sensitivity and the probe polarization, then AutoCapture will function reliably.
Le passage par un test de configuration est nécessaire pour confirmer que le système
AutoCapture fonctionne avec la sonde implantée (capacité à bien différencier le signal
correspondant à la capture et le signal de perte de capture).
- Ce test mesure la réponse évoquée et l’artéfact de polarisation pour permettre une évaluation efficace de la capture
- S’il existe une marge de sécurité suffisante entre le signal de réponse évoquée (capture) et la polarisation de la sonde, alors le fonctionnement de l’AutoCapture est fiable
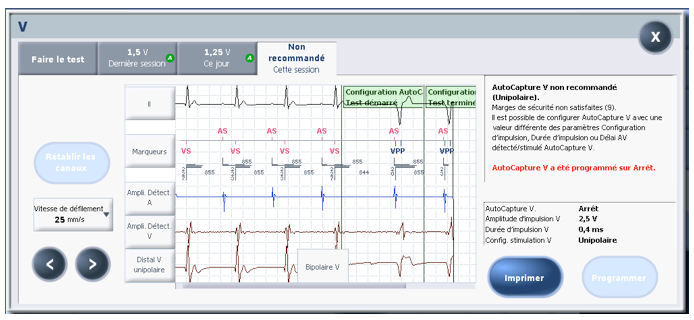
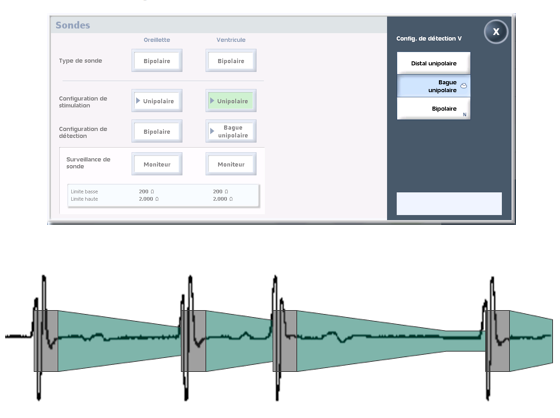
At the end of the configuration test, the device indicates whether AutoCapture is recommended or not recommended.
Configuration test result: not recommended in this example for bipolar detection and unipolar stimulation. The option remains to change the detection and stimulation mode (Zephyr range and above) and/or the pulse duration, then rerun the test.
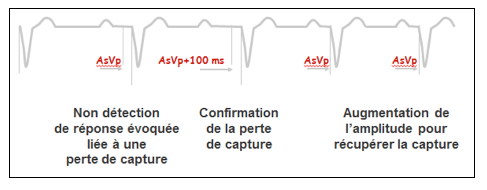
2 – Recovery from loss of capture
If the capture check confirms two consecutive losses of capture, the device initiates the loss of capture recovery algorithm. In the next cycle, the pacemaker delivers a rescue pulse, then increases the automatic pulse amplitude by 0.25 V and searches for capture. If no capture is confirmed, the device increases the pulse amplitude by 0.125 V in the next cycle and searches for capture. When two successive captures are confirmed at the same voltage, the device begins a threshold search.
If no capture is confirmed before the device automatically increases the pulse amplitude to 3.875 V, the device switches to High Amplitude Mode: the pulse amplitude is set to 5 V and the pulse duration to 0.5 ms (or more if the programmed value is higher). After 128 cycles, the device begins a threshold search.
Récupération de la perte de capture
Cet algorithme permet une adaptation de l’amplitude s’il y a détection d’une perte de
capture. Si le dispositif met en évidence deux pertes de capture consécutives, il active
l’algorithme de récupération de perte de capture.
- Le cycle suivant, le stimulateur délivre une impulsion de secours puis augmente l’amplitude d’impulsion automatique de 0,25 V et recherche une capture
- Si aucune capture n’est confirmée, l’appareil augmente l’amplitude d’impulsion de 0,125 V sur le cycle d’après et recherche la capture
- Lorsque deux captures successives sont confirmées à la même tension, l’appareil commence une recherche du seuil
- Si aucune capture n’est confirmée pour une amplitude d’impulsion à 3,875 V, l’appareil commute sur Mode haute amplitude ; l’amplitude d’impulsion est réglée sur 5 V et la durée d’impulsion sur 0,5 ms (ou plus si la valeur de programmation est supérieure) ; après 128 cycles, l’appareil
commence une recherche du seuil
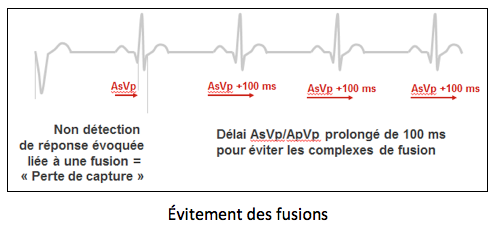
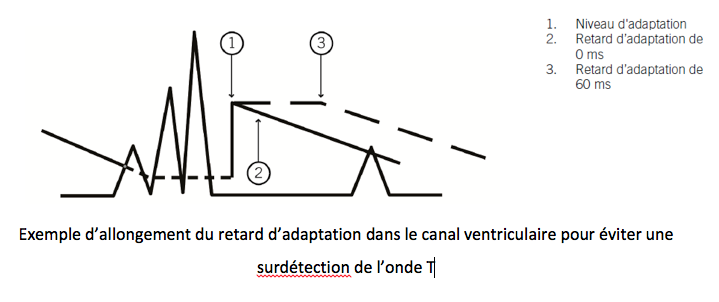
3 – Avoiding mergers
Mergers with AutoCapture should be avoided because the algorithm would conclude that there has been a loss of capture due to an increase in the threshold and would trigger its capture loss recovery algorithm.
In dual-chamber mode, a single absence of ER detection, requiring the delivery of a 5 V rescue pulse, automatically causes the stimulated and detected AV delay to be extended by 100 ms during the next cycle in order to search for spontaneous conduction. As a first step, the algorithm “assumes” that the capture loss is due to fusion and not to a lack of pulse energy. This function acts in a similar way to VIP.
If capture loss is confirmed after the stimulated or detected AV delay is extended (two consecutive cycles requiring the delivery of a 5 V safety pulse), the pacemaker triggers its capture recovery algorithm:
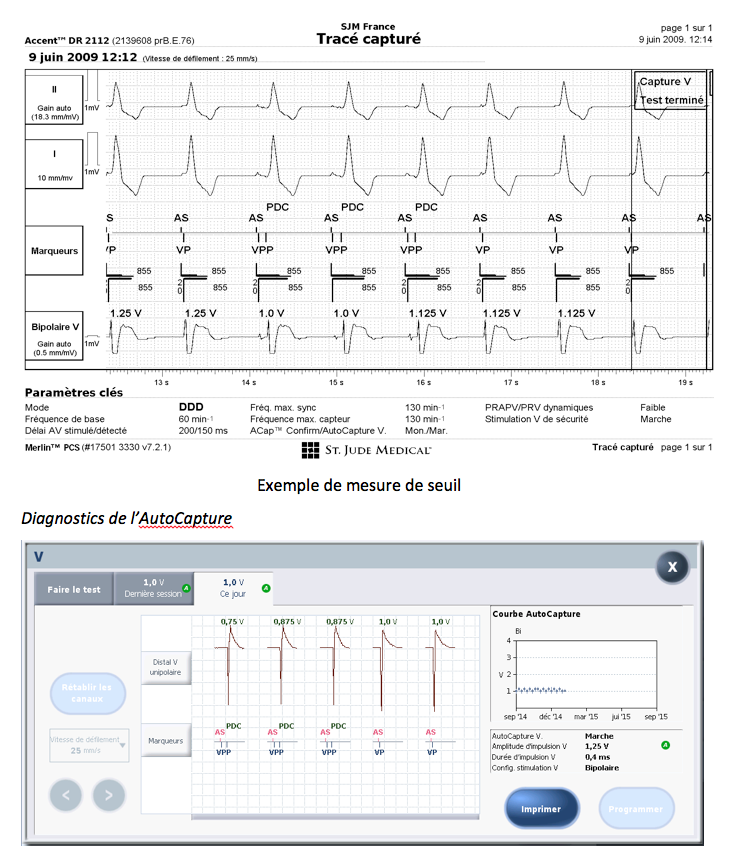
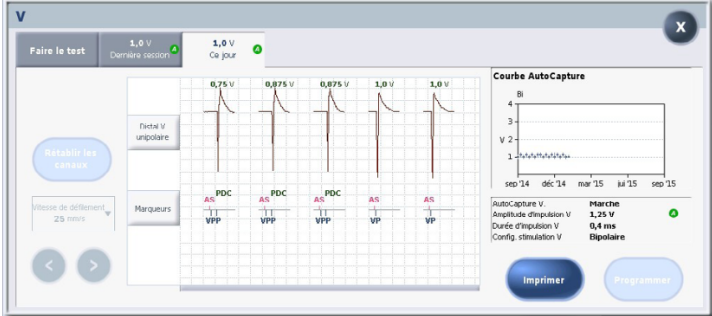
Diagnostics de l’AutoCapture
- Courbe de tendance qui affiche l’évolution du seuil sur un an
- EGM enregistré qui correspond au seuil le plus récent
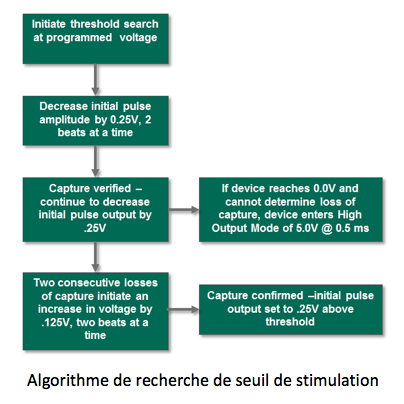
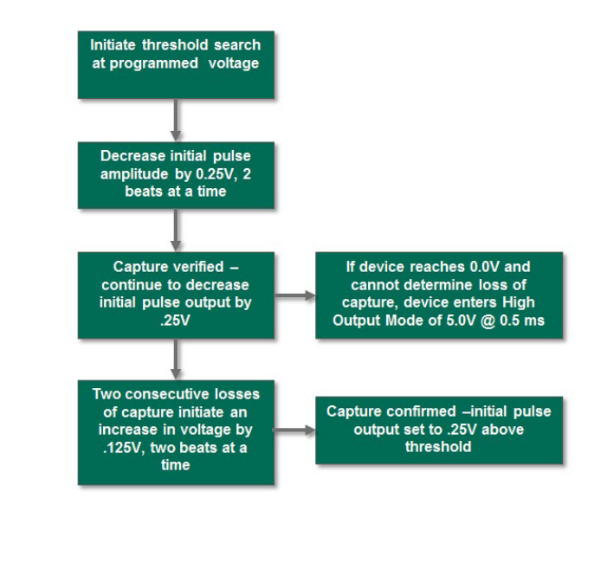
4 – Periodic measurement of the stimulation threshold
When automatic threshold search is initiated (every 8 or 24 hours), the device decreases the pulse amplitude by 0.25 V every two cycles. If this leads to a loss of capture, the device emits a backup pulse of 5 V (safety margin) 80 to 100 ms after the first test pulse. If capture is lost on two consecutive cycles at the same amplitude, the algorithm then increases the pulse amplitude in steps of 0.125 V every two cycles. Two consecutive captures at the same amplitude must be confirmed to determine the new stimulation threshold value. When this is found, the device determines a new Automatic Amplitude by adding a working margin of 0.25 V.
If the descending search fails to determine a loss of capture at the lowest pulse amplitude setting, i.e., 0 V, the device switches to “High Amplitude Mode” for a period of 128 cardiac cycles, then restarts the threshold search.
If the stimulation threshold determined by the algorithm exceeds 3.875 V for a certain pulse duration, AutoCapture is automatically disabled and the pulse amplitude is reprogrammed to 5 V (High Amplitude Mode). A higher pulse duration setting may allow AutoCapture to be reactivated in this case.
Threshold searching is repeated 1) after each capture loss recovery operation 2) automatically every 8 hours 3) when the telemetry head is removed 4) when the magnet is removed 5) when the operator performs the stimulator threshold test via Autocapture™.
To avoid mergers, the stimulated AV Delay is programmed to 50 ms and the detected AV Delay is programmed to 25 ms. The programmed values are restored when the search is complete.
Trend line showing the change in the threshold over one year
Recorded EGM corresponding to the most recent threshold
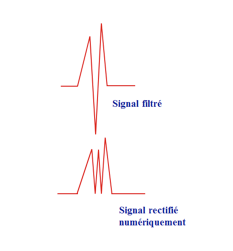
Sensing
After filtering, the signal is also digitally rectified. Detection is based on a single-phase signal.
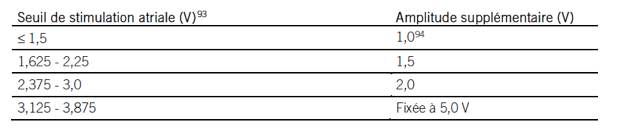
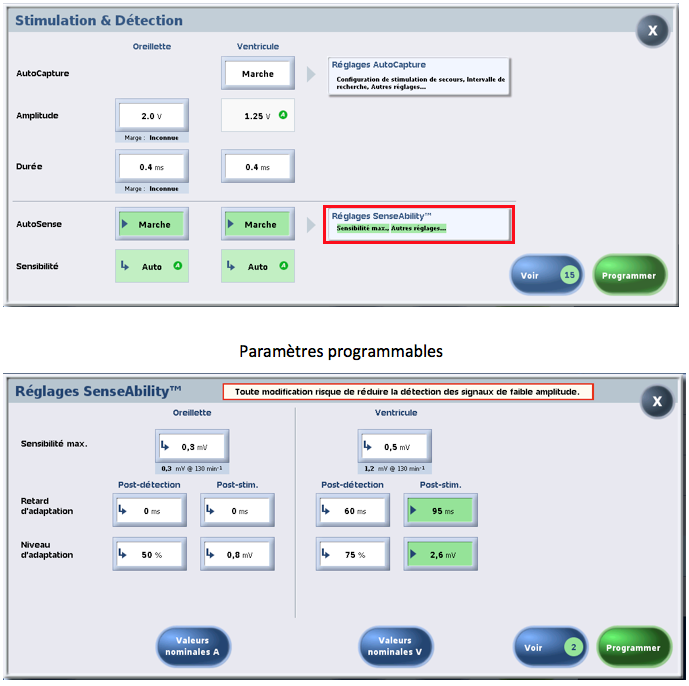
In bipolar detection, atrial and ventricular sensitivity can be programmed to automatic (AutoSense or SenseAbility) or fixed. However, sensitivity must be fixed if detection is unipolar. When the lead is coded as bipolar, unipolar detection can be programmed either between the distal tip and the pacemaker body or between the ring and the pacemaker body.
The principle of automatic sensitivity control is to adjust sensitivity based on the amplitude of the previous P wave or R wave and then increase sensitivity during the cycle. Maximum bipolar sensitivity is limited to an adjustable value (0.2 mV in the atrium nominally and 0.5 mV in the ventricle).
Various parameters can be programmed to optimize detection quality: maximum sensitivity, adaptation delay (post-stimulation and post-detection), adaptation level (post-stimulation and post-detection), and stimulated and detected refractory period (post-stimulation and post-detection).
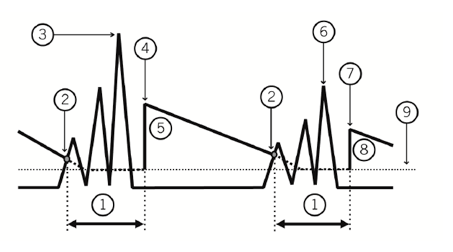
In the example in the figure below, the device detects an R wave measured at 6 mV. At the end of post-detection blanking, the sensitivity is initially set to the adaptation level (in this example, 50% of the maximum measured signal; 3 mV). This sensitivity level is maintained during the adaptation delay (in this example, no adaptation delay; 0 ms). The sensitivity then increases linearly until the next detected event or until the maximum sensitivity (1 mV in this example).
1. Post-detection blanking; 2. R wave detected; 3. Maximum amplitude of R wave: 6 mV; 4. Adaptation level set to 50%; 5. Sensitivity at 3 mV; 6. R wave at 4 mV; 7. Adaptation level set to 50%; 8. Sensitivity at 2 mV; 9. Maximum sensitivity;
When the post-ventricular pacing delay is set to Auto, the device automatically adjusts the delay used after a ventricular pacing to compensate for the shortening of the QT interval associated with rapid pacing rates.