Tracé 7.14: Maladie d’ebstein, pré-excitation et fibrillation auriculaire
Patient information
28-year-old man with Ebstein’s disease with pre-excitation; at the age of 11, the patient underwent a first procedure for the removal of a right posterolateral accessory pathway responsible for palpitations; current emergency hospitalization for sudden palpitations with unstable hemodynamics; injection of 2 ampules of intravenous amiodarone allowed a reduction of the arrhythmia with clinical stabilization;
ECG
Question
What is(are) the possible diagnosis(es) on this ECG?
Comments
ECG description
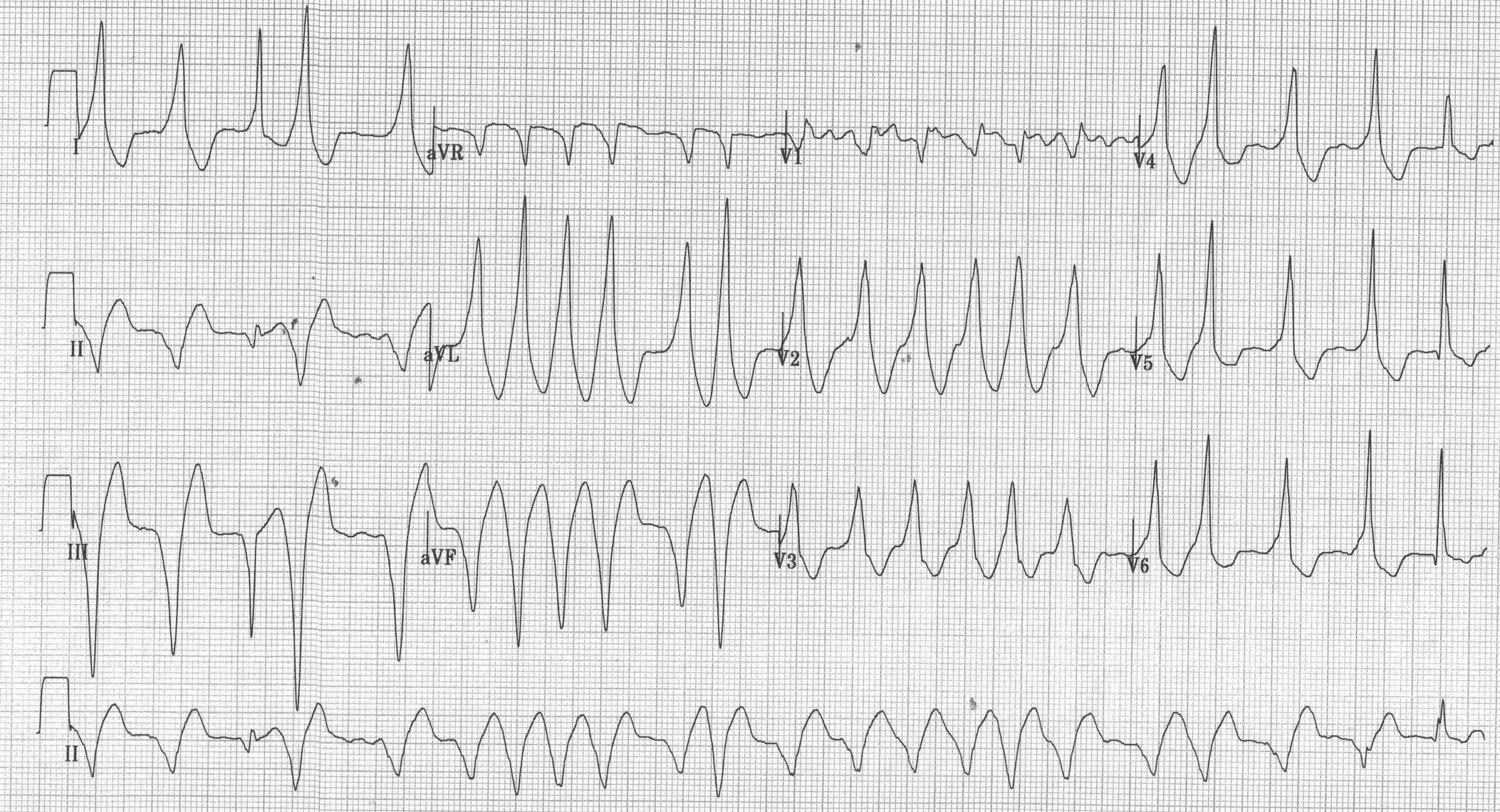
ECG recorded on arrival; irregular and rapid ventricular rhythm (shortest RR measured at 230 ms); accordion-like pattern characteristic of atrial fibrillation due to ventricular pre-excitation; when the QRS complexes are maximally pre-excited (broadest QRS), we observe a left axis, a QS pattern in V1 and a transition between V1 and V2; the electrocardiographic pattern is characteristic of an atrial fibrillation due to accessory pathway;
Explanation
Patients with Ebstein’s disease frequently have not only one or more accessory pathways but also an increased incidence of atrial arrhythmias in conjunction with either a tricuspid regurgitation, a major dilatation of the right atrium or a possible surgical scar. The association between atrial fibrillation and a permeable accessory pathway can be particularly threatening.
Treatment of the accessory pathway is dependent on the presence of arrhythmias, their frequency, their severity and the degree of permeability of the accessory pathway. A class IC anti-arrhythmic treatment can be proposed. The cut-off limit separating low-risk patients who only require medical treatment and high-risk patients requiring ablation of the accessory pathway is difficult to define. For this patient presenting episodes of atrial fibrillation with rapid conduction via the accessory pathway leading to a precarious hemodynamic state, ablation appears indispensable. In patients with little or no symptoms, the preferred therapeutic approach is of greater debate. However, the benign or malignant nature should probably be systematically assessed.
The ablation procedure can be technically difficult with a lower success rate than for an accessory pathway in a healthy heart. Indeed,
1. as explained previously, a same patient may have multiple pathways; these accessory pathways may be long and of significant diameter;
2. the delineation between atrial myocardium and ventricular myocardium is less straightforward and the presence of abnormal, fragmented signs unrelated to the accessory pathway at the atrial level is frequently observed;
3. the right atrium is often very dilated, rendering the manipulation of catheters difficult and requiring the use of sheaths with large curvatures;
4. obtaining high temperatures is sometimes difficult;
5. the aggressiveness of the lesions must sometimes be limited, due to the description of lesions of the right coronary artery.

Trace description
This patient underwent a successful ablation procedure of a right posterolateral accessory pathway; characteristic pattern of Ebstein’s disease: sinus rhythm, right atrial enlargement, prolonged PR interval (first degree atrioventricular block in relation to a prolonged right atrial depolarization time); incomplete right bundle branch block;
To remember
Patients with Ebstein’s disease are at increased risk of sudden death due to the presence of one or more accessory pathways but also with an increased incidence of atrial arrhythmias.