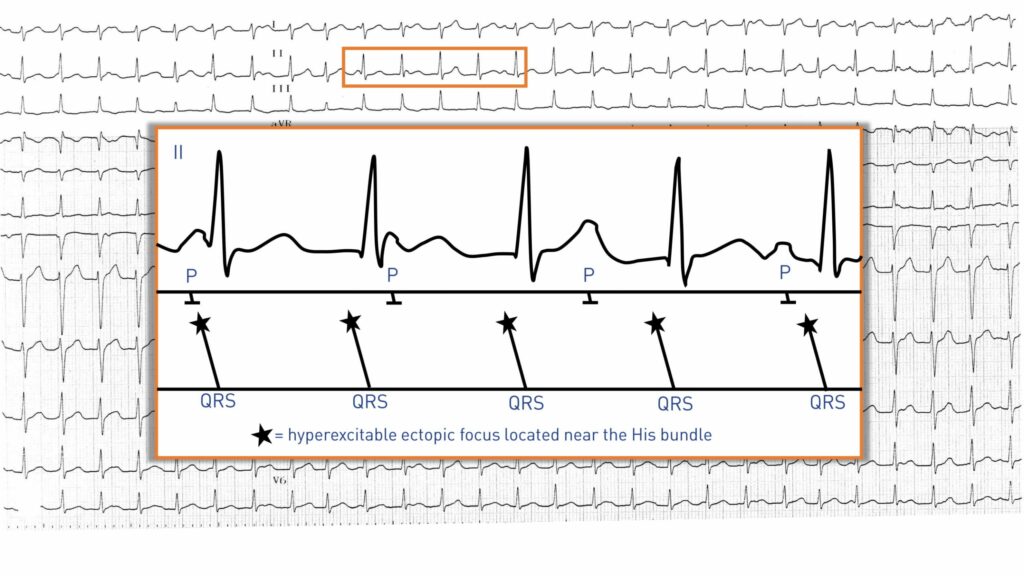
This tracing was recorded during the sensation of palpitations; tachycardia of 140 bpm, narrow QRS with atrioventricular dissociation; QRS complexes without any particular abnormality are found with a sinus atrial activity (identifiable P wave, positive in leads I, II and negative in aVR) that is slower and dissociated from ventricular activity; these elements are indicative of a junctional ectopic tachycardia; atrial activity is normal and sinus, which allows eliminating the hypotheses of atrial fibrillation or flutter; atrial and ventricular activities are dissociated, which eliminates reentry due to an accessory pathway (mandatory 1:1 ratio between atria and ventricles); the probability of an intranodal reentry with dissociated atrial activity is very low;
Junctional ectopic tachycardia (JET) is a rare arrhythmia associated with an ectopic focus of hyperexcitability located at the level of the bundle of His. This type of arrhythmia has been described in the context of digitalis poisoning or myocardial ischemia although it is usually found in two other distinct situations.
1. in the aftermath of cardiac surgery for the repair of congenital heart disease. A junctional ectopic tachycardia primarily occurs 24 to 48 hours after closure of an interventricular communication, is generally transient in this setting and most often disappears within one week. However, the tachycardia can complicate both the surgical procedure and the stay in intensive care unit by increasing the risk of cardiac decompensation. Various therapeutic strategies have been proposed in this setting (amiodarone, rapid atrial pacing or hypothermia, reduction of central temperature to reduce hyperexcitability);
2. a much more severe primitive form in infants or children with healthy hearts. The congenital form was initially described by Coumel with description of family cases. The arrhythmia occurs during the first 6 months of life and is mostly quasi-permanent. It can predispose to the occurrence of cardiomegaly and heart failure, with mortality being non-negligible (atrioventricular block or ventricular fibrillation episodes). Autopsy analyses reveal a severe disruption in the organization of the bundle of His fibers, which explains the occurrence of arrhythmia but also of conduction disturbances.
The electrocardiogram reveals certain characteristic elements:
• A tachycardia with a rate between 160 and 300 bpm; Holter-ECG analysis may show moderate rate variations over 24 hours
• Narrow QRS complexes even with the possibility of a conduction aberration
• Atrioventricular dissociation; the ECG typically shows a tachycardia with retrograde conduction block (presence of a dissociated sinus activity). This allows formally excluding tachycardias originating from the atria or reentrant tachycardias due to an accessory pathway. Sometimes, as on the second tracing, there is a retrograde conduction (negative P’ waves in inferior leads). In much rarer instances, an anterograde block can be observed with no conduction to the ventricles along with missing QRS complexes.
When the onset of an arrhythmia episode is recorded, a warm-up phenomenon with a gradual acceleration of the rate is frequently observed. The arrhythmia begins with a junctional extrasystole followed, without echo phenomenon, by other identical extrasystoles which interconnect with increasing frequency to reach a stable rate. A cooling phenomenon (gradual deceleration of the rate) can also be observed at the end of the episode.
The diagnosis can be confirmed in the electrophysiology laboratory with the inability to induce or reduce the arrhythmia by atrial/ventricular pacing (as opposed to reentrant tachycardia) or by electric shock. Injection of Adenosine does not interrupt tachycardia but may block retrograde conduction when there is a 1:1 ratio. The tachycardia thus persists with a dissociation which allows eliminating the differential diagnosis of reentrant tachycardia due to accessory pathway. A prolonged atrial pacing faster than the tachycardia rate can capture the conduction pathways and restore atrioventricular synchronism.
Commentary
The evolution can be marked by a spontaneous extinction of this hyper-excitability focus in the bundle of His. Treatment is indicated when the rate is rapid, when the patient is symptomatic or upon occurrence of signs of heart failure. Different therapies can be proposed over the long term:
- drug treatments; the results are often less that optimal and it should be reminded that each of these antiarrhythmic treatments is associated with a non-negligible risk of side effects, especially since these treatments must be maintained for prolonged periods with large dosages. Amiodarone appears to provide the best results, although a combination therapy with flecainide is sometimes necessary for refractory forms;
- ablation of the pathological arrhythmogenic area by surgery or by radiofrequency may be curative. The objective is to eliminate the culprit focus while preserving atrioventricular conduction to avoid the need for pacemaker implantation;
- it may be decided to implant a pacemaker in the context of the occurrence of a complete spontaneous atrioventricular block or induced by an ablation of the bundle of His.
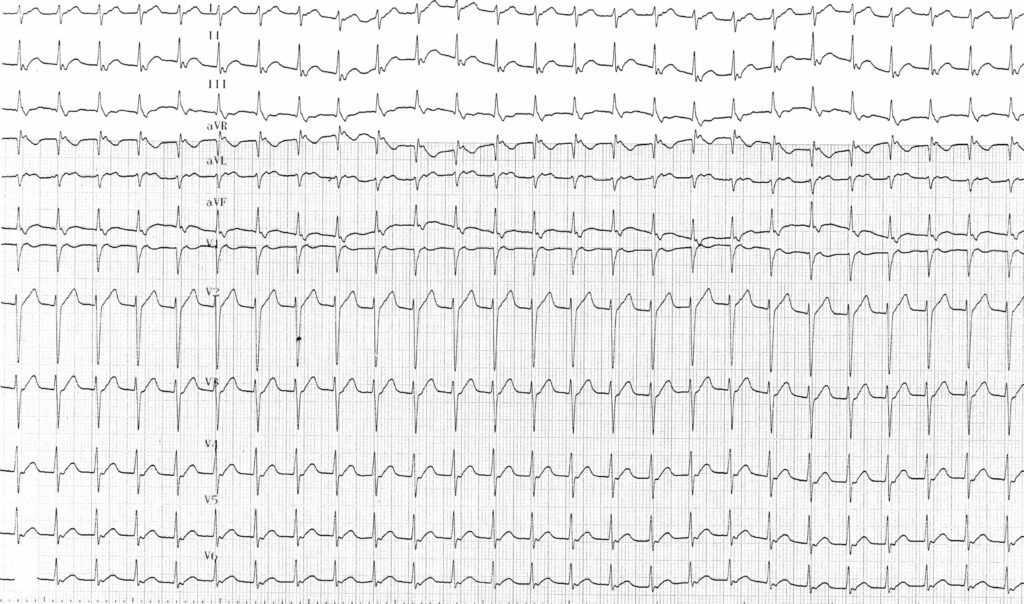
Trace description
Tracing recorded a few minutes later with, in this instance, a retrograde conduction to the atria (negative P waves in inferior leads) and a 1:1 ratio;
Une tachycardie jonctionnelle ectopique se traduit généralement sur l’électrocardiogramme par une tachycardie à QRS fins (fréquence entre 160 et 300 bpm) avec dissociation auriculo-ventriculaire;


