

Trace description
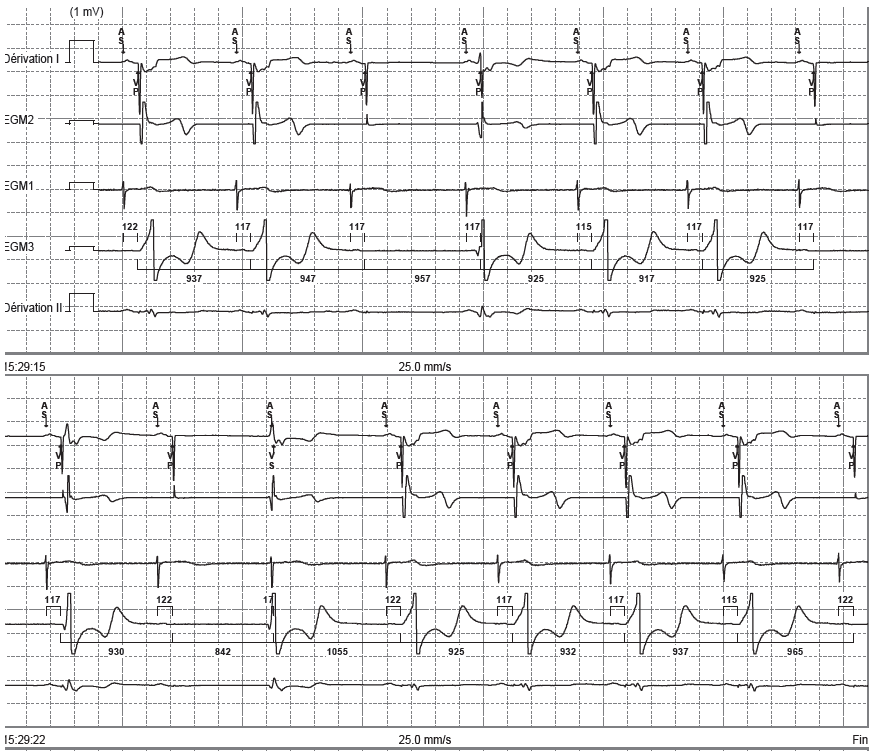
The EGM confirms the absence of ventricular capture with an extra beat and junctional escape;
Trace description
A recording that continues from the first one; an increase in the number of ineffective ventricular pacing events;
Commentary
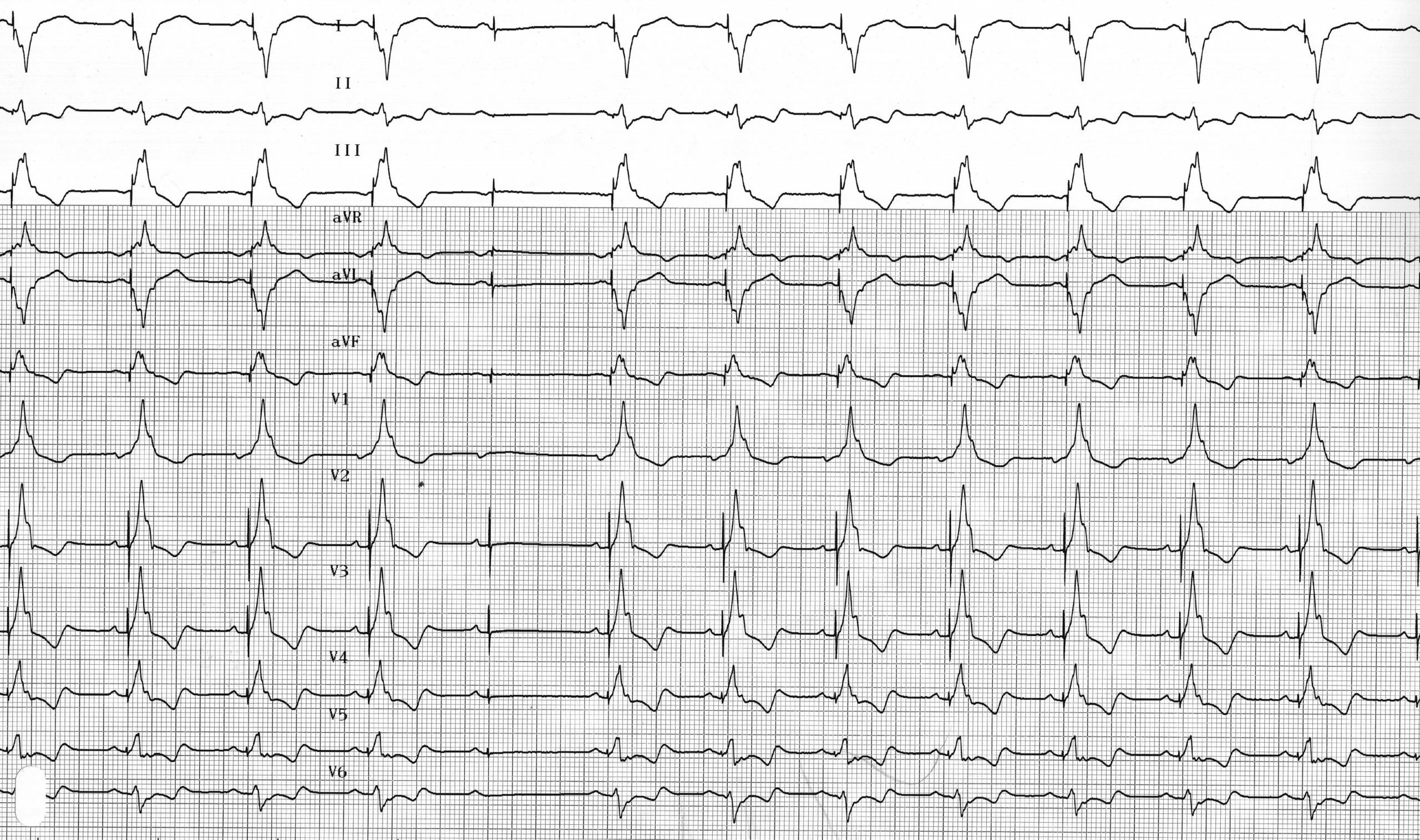
These tracings demonstrate intermittent ventricular capture loss in a patient with a dual-chamber pacemaker implanted due to complete atrioventricular block and who is therefore dependent on the pacemaker. Intermittent capture loss due to an elevated ventricular pacing threshold leads to syncope with a high risk of sudden death.
The pacing threshold is the smallest electrical impulse, delivered outside of all natural refractory periods, capable of triggering the propagation of depolarization. It can be measured in voltage (volts) or pulse width (milliseconds). Determining the pacing threshold is of major importance, as programming the voltage and pulse duration establishes the safety margin and determines the device’s energy consumption—and thus the rate at which the batteries wear out. It is generally recommended to program a safety margin of 100%, which corresponds to a voltage twice the threshold. This safety margin is intended to account for circadian variations in the stimulation threshold, which can vary from person to person due to factors such as sleep, meals, physical activity, fever, and so on.
Today, all modern pacemakers can be programmed with a function for automatic measurement of the ventricular threshold, which may or may not be combined with automatic adjustment of the pacing amplitude and cycle-by-cycle verification of capture efficiency (Autocapture allows for the delivery of amplitudes very close to the threshold, with high-amplitude safety pacing in the event of loss of capture) or adaptation over extended periods following scheduled threshold testing but without cycle-by-cycle verification (Autocapture, which requires larger safety margins). For the five major manufacturers, assessment of ventricular capture is based on analysis of the evoked response (distinguishing between polarization and evoked response). For Biotronik, Boston Scientific, and St. Jude Medical pacemakers, there is cycle-by-cycle monitoring of ventricular capture efficacy, allowing for the delivery of amplitudes very close to the measured threshold. For Medtronic and Sorin pacemakers, the threshold is measured periodically, with the amplitude adjusted based on this measurement, but without cycle-by-cycle verification of capture, requiring larger safety margins.
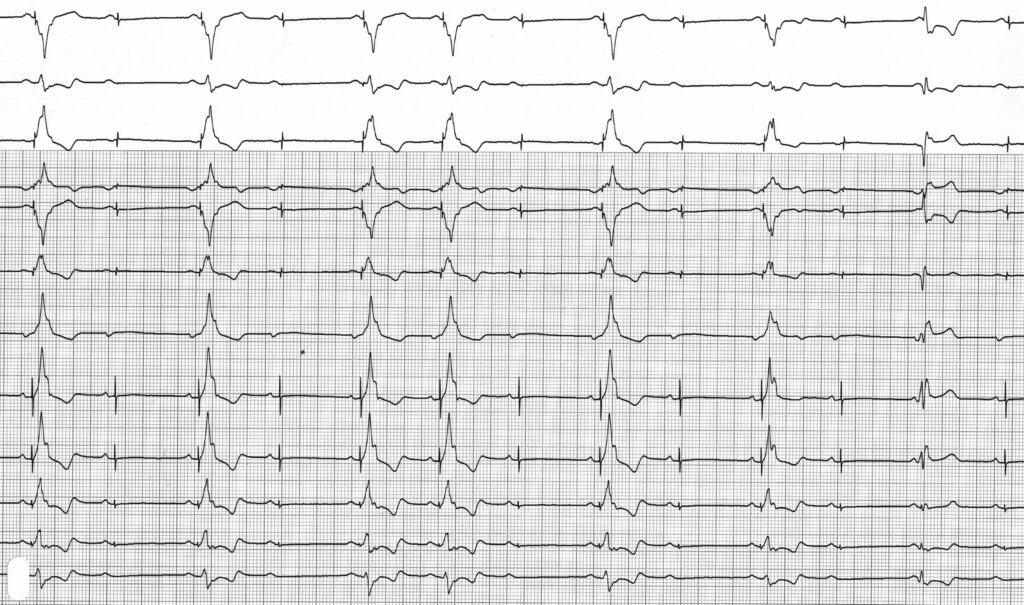
This patient benefited from an increase in pacing amplitude (from 2.5 to 4 volts for a threshold of 2.6 V), which eliminated the symptoms.

Trace description
The test confirms the elevation of the right ventricular threshold; this trace was recorded after increasing the pacing amplitude and shows sustained effective capture;