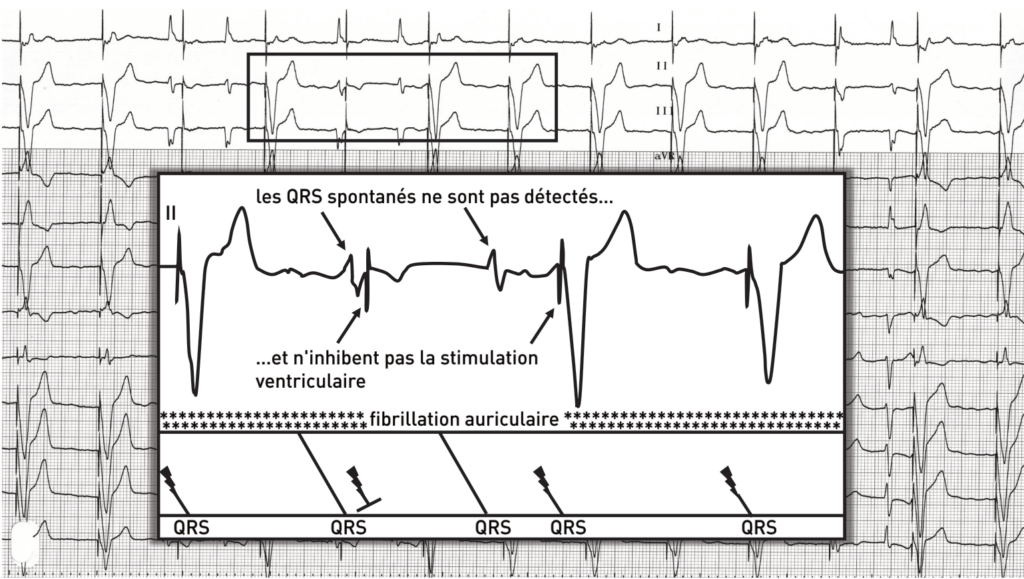
This trace reveals ventricular underdetection, which can sometimes lead to pacing during the vulnerable period. In the absence of proper detection, the pacemaker operates in asynchronous mode, making it impossible to inhibit spontaneous ventricular contractions. There is a low but non-zero theoretical risk of inducing a malignant polymorphic ventricular arrhythmia that could compromise the patient’s survival. Furthermore, this unnecessary pacing leads to energy consumption that is detrimental to the device’s lifespan.
Sensitivity, expressed in millivolts (mV), describes the pacemaker’s ability to correctly detect spontaneous cardiac events. A pacemaker is equipped with input filters that specifically detect P waves in the atrium and R waves in the ventricle based on the analysis of three characteristics of these electrical signals: the frequency spectrum, the slope, and the amplitude.
Proper sensitivity level programming should allow for the detection of all spontaneous cardiac events occurring in the implanted chamber while avoiding the detection of events of other types (crosstalk with detection of cardiac signals from the other chamber, myopotentials, interference, etc.). Programming for bipolar detection increases detection specificity compared to unipolar detection by limiting the risk of picking up extracardiac signals or cross-talk, and allows for the programming of high sensitivity values. In contrast, in a unipolar configuration, the risk of cross-sensing or picking up extracardiac signals necessitates programming a lower sensitivity level, which carries an increased risk of underdetection.
Traditionally, unlike defibrillators, pacemakers operated with a stable, fixed sensitivity throughout the cardiac cycle. Increasingly, even though the detection requirements are not the same (it is crucial for a defibrillator to detect and treat very rapid, polymorphic, and microvolt ventricular arrhythmias), modern pacemakers offer adaptive sensitivity (a sensitivity level that varies depending on the amplitude of the detected R-wave or P-wave) with a gradual increase in sensitivity over the course of the cardiac cycle (allowing for the detection of low-amplitude signals without overdetecting the T-wave).
Programming a more appropriate adaptive ventricular sensitivity resolved the issue in this patient.