

The vast majority of pacemaker leads implanted today in the right atrium or right ventricle are bipolar. On a bipolar lead, it is possible to program the pacing and sensing configuration to be either unipolar or bipolar. All pacing circuits are, by definition, bipolar, with an electron flow directed from the cathode to the anode. The term “unipolar pacing” is technically incorrect and refers to the fact that a single electrode is located at the tip of the lead in contact with the heart, with the pacemaker housing serving as the other electrode in the circuit. In bipolar pacing, both electrodes of the circuit are located at the tip of the lead within the heart, with a limited inter-electrode distance.
Certain factors support the choice of a unipolar pacing configuration. The unipolar pacing threshold is generally very slightly lower than that for bipolar pacing due to a slightly lower total resistance of the pacing system (larger anode). The stimulation artifact is more easily identifiable because it has a higher voltage (at equal amplitude) during unipolar stimulation than during bipolar stimulation. The size of the stimulus in unipolar mode facilitates interpretation of the trace, especially if the physician or nurse is unaware that the patient has a pacemaker.
The limitations of unipolar pacing stem from the fact that, because the pacing field is wider and includes the device housing, the risk of pectoral pacing within the pocket and the risk of cross-sensing (detection of atrial pacing by the ventricular channel and vice versa) are significantly increased.

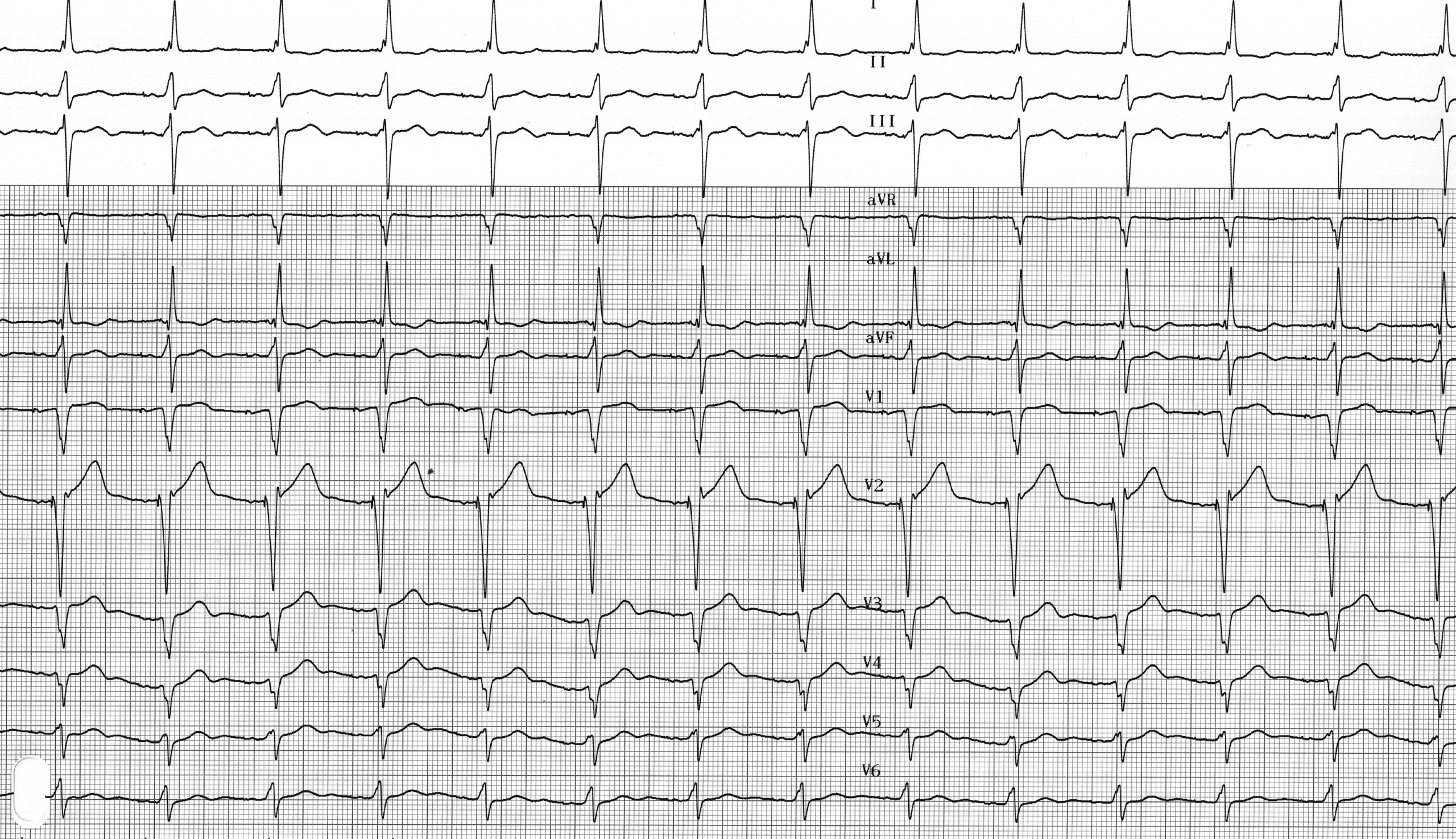
Trace description
Same trace, but atrial and ventricular pacing in unipolar mode;