Abbott - AV delay, PMT, refractory periods
Content
Atrial refractory period
Blanking and post-atrial refractory period
There is a programmable post-atrial detection refractory period (between 93 and 190 ms, nominal value 93 ms).
Similarly, after atrial pacing, there is a programmable atrial refractory period (between 190 and 470 ms, nominal value 190 ms).
Events occurring during this refractory period are not taken into account for the counting of atrial arrhythmias (calculation of the filtered atrial rate).
Post-ventricular atrial refractory periods
1. Post-ventricular atrial blanking
Following ventricular pacing, there is atrial blanking of 60 to 250 ms (nominal value, 150 ms). Events occurring during this refractory period are not counted toward the atrial arrhythmia count (filtered atrial rate calculation).
2. Post-ventricular atrial refractory period (PVARP)
The PVARP is programmable between 125 and 500 ms (nominal value 275 ms).
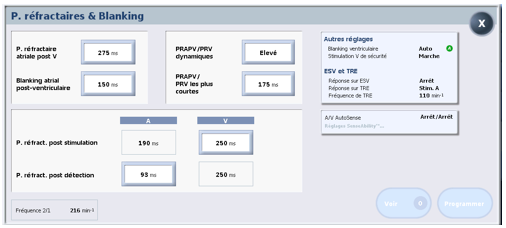
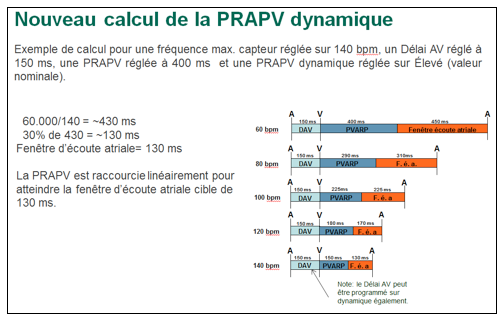
Programming a dynamic PVARP allows the PVARP value to be adjusted according to heart rate. This parameter can be set to Off, Low, Medium, or High. The shortest PVARP must also be programmed (programmable between 125 and 475 ms, nominal value 175 ms).
Ventricular refractory period
Blanking and post-ventricular ventricular refractory period
After ventricular pacing, there is a programmable ventricular refractory period (between 125 and 470 ms, nominal value 250 ms).
Similarly, there is a programmable post-detection ventricular refractory period (between 125 and 500 ms, nominal value 250 ms).
Post-atrial stimulation ventricular refractory periods
1. Post-atrial stimulation ventricular blanking
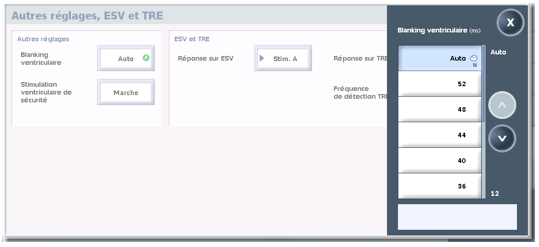
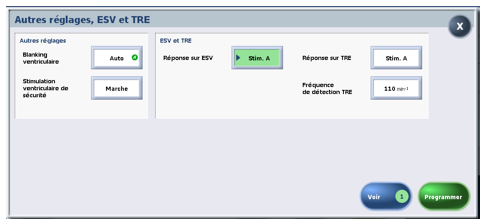
This blanking can be programmed to AUTO (from the Accent platform at nominal value) or to a fixed value between 12 and 52 ms. When AUTO programming is selected, if a ventricular signal is detected during blanking, blanking is automatically extended until no signal is detected or until the limit value of 52 ms is reached.
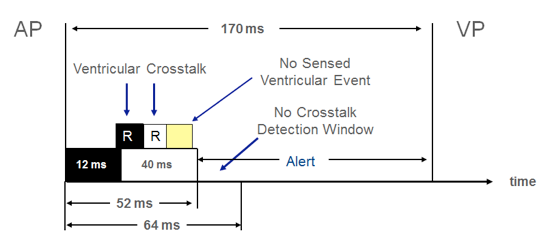
2. Ventricular safety pacing
The safety window can be programmed to be on or off (default setting is on). If a ventricular signal is detected within the safety window (which begins after ventricular blanking following atrial pacing and ends 64 ms after the atrial stimulus), ventricular pacing is triggered 120 ms after atrial pacing.
If post-atrial ventricular blanking is programmed to “Auto”:
- if a ventricular signal is detected during the initial 12 ms blanking period (possible cross-listening), new 12 ms re-triggerable blanking periods follow one another until detection stops, without exceeding a limit set at 52 ms;
- if ventricular detection ends before this 52 ms limit, the cross-listening window is interrupted; if ventricular detection occurs before the end of the AV delay, ventricular pacing is inhibited; if no detection occurs, ventricular pacing occurs at the end of the AV delay;
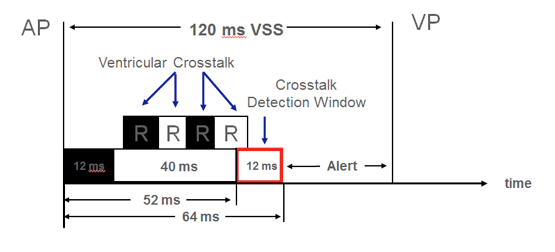
- if ventricular detection continues beyond this 52 ms limit (start of the safety window), ventricular pacing is delivered 120 ms after atrial pacing;
Pacemaker mediated tachycardia
Preventing PMT initiation
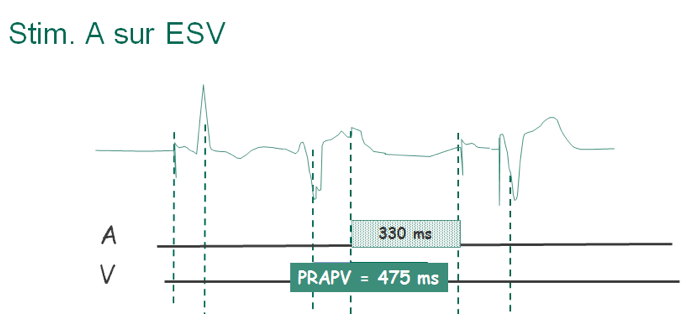
To avoid stimulating the atrium during vulnerable periods, Abbott pacemakers maintain a fixed interval of 330 ms before stimulating the atrium, regardless of the programmed or servo frequency.
If the Response on PVC setting is set to Stim. A (other setting: Off), detection of a PVC causes the PVARP to be extended to 475 ms. Atrial pacing can only occur 330 ms after detection of atrial activity in the PVARP.
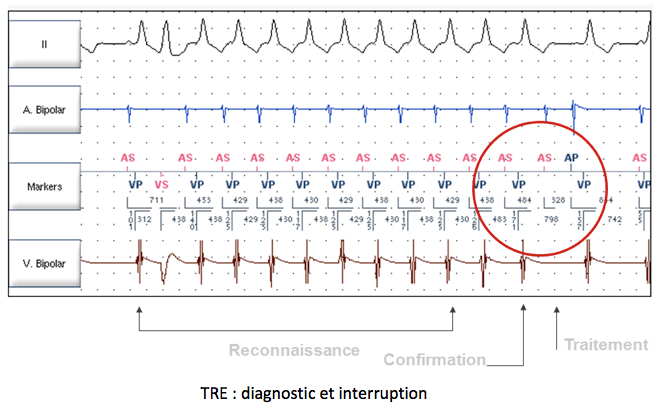
Diagnosis of a PMT by the pacemaker and anti-PMT intervention
To prevent a PMT from becoming permanent, Abbott pacemakers have a recognition and treatment algorithm based on the stability of the VP interval.
There are three possible settings for the response to PMT:
- Off: no PMT detected;
- Passive: PMTs are detected and included in the diagnostics, but the interruption algorithm is not used;
- Atrial pacing: PMTs are detected and the specific interruption algorithm is used;
The PMT detection rate parameter determines how often the device checks for tachycardias compatible with PMT. This parameter can be set between 90 and 150 bpm (nominal value 130 bpm) and cannot exceed the maximum synchronous rate value.
If the VP interval is stable over 8 cycles, the PV delay is modified by 50 ms (shortened by
50 ms if the AS-VP interval is > 100 ms, lengthened by 50 ms if the AS-VP interval is < 100 ms) on the ninth cycle.
If the VP of the tenth cycle is unchanged (less than 16 ms variation from the previous VP), the P wave is considered retrograde and does not synchronize ventricular pacing.
Atrial pacing is delivered 330 ms after P’.
If the ninth and tenth VP intervals differ by more than 16 ms, the device concludes that there is no PMT; the search for PMT only resumes after 256 cycles.