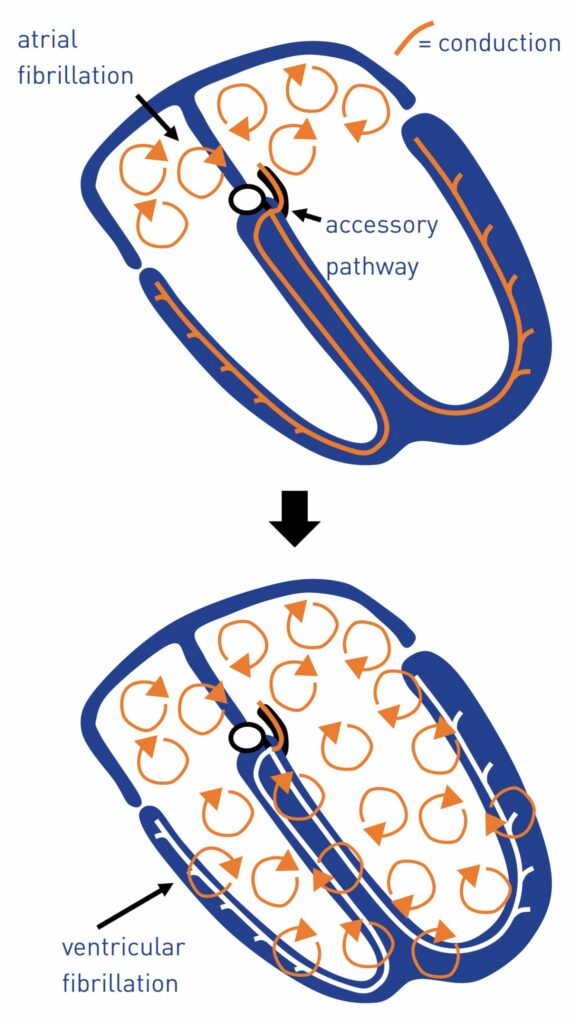
Wolff-Parkinson-White syndrome is sometimes considered benign and treatment is usually proposed in symptomatic patients with episodes of reciprocating tachycardia. However, as seen previously, the incidence of atrial fibrillation is high despite the absence of obvious signs of organic heart disease. The occurrence of this type of arrhythmia can burden the patient’s life-threatening risk, a very rapid ventricular response on a very permeable accessory pathway (very short anterograde refractory period) potentially degenerating into lethal ventricular fibrillation.
The difficulty of managing patients with an accessory pathway lies in the fact that an episode of rapid atrial fibrillation leading to sudden death may be the first disease expression and occur in a previously asymptomatic patient. Identifying at-risk patients remains difficult even though it is recognized that the risk of sudden death is greatest in patients with a very short anterograde refractory period (less than 220 ms).
When faced with a patient with an atrial fibrillation episode due to accessory pathway, the curative treatment is based on emergency cardioversion if hemodynamics are unstable, or class IC antiarrhythmic agents or amiodarone if hemodynamics are preserved. On the other hand, drugs blocking nodal conduction and not slowing conduction through the accessory pathway (adenosine, calcium channel blockers, beta-blockers, digitalis) are formally contraindicated.
The presence of pre-excited QRS with very short RR cycles during electrophysiological study or the presence of an episode of atrial fibrillation that is poorly supported clinically constitute an indisputable indication for radiofrequency ablation.
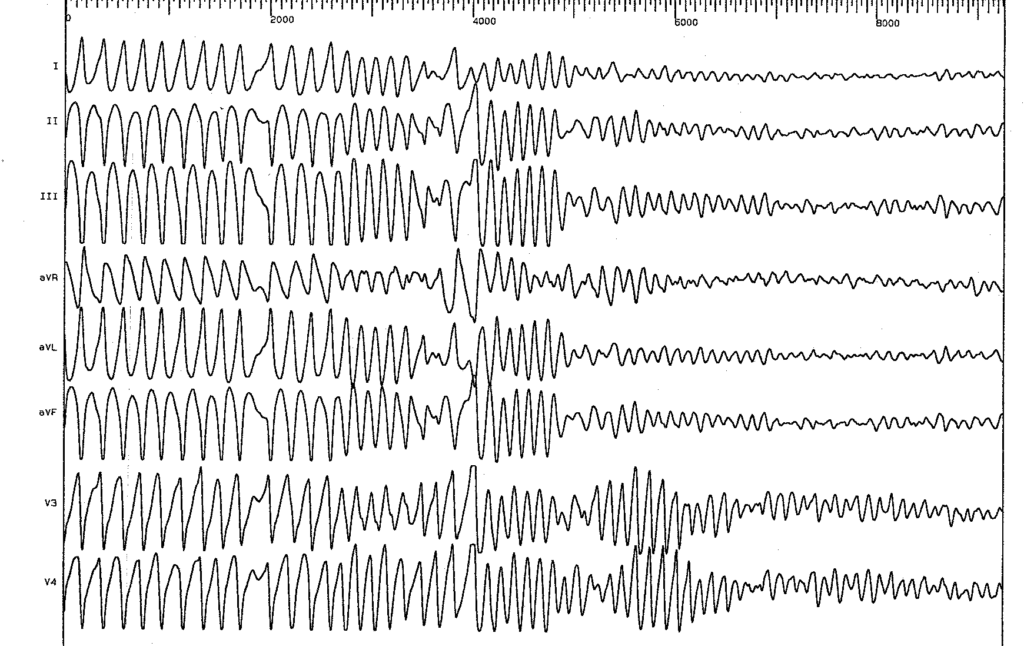
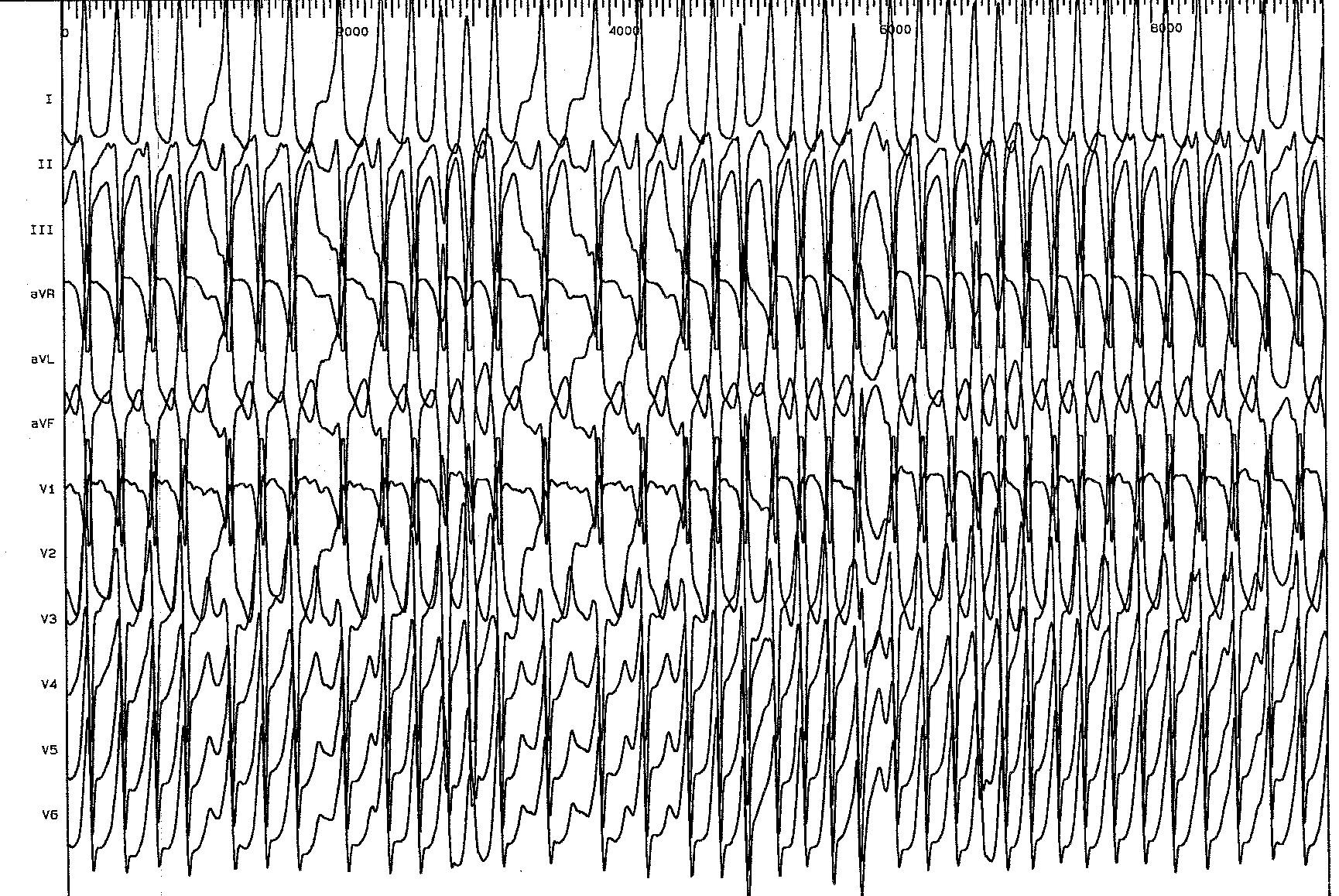
Trace description
Extremely short RR cycles; in the second part of the tracing, the rhythm degenerates into ventricular fibrillation (disorganized activity); loss of consciousness of the patient; an electric shock is thus necessary to restore an effective sinus rhythm;