Trace 4.11: Lack of fall-back algorithm for atrial arrhythmia
Patient information
A 78-year-old man with a dual-chamber pacemaker implanted due to atrial disease; admitted to the hospital for palpitations and signs of cardiac decompensation
ECG
Question
Regarding this ECG, which of the following is/are the correct answer(s)?
Comments
ECG description
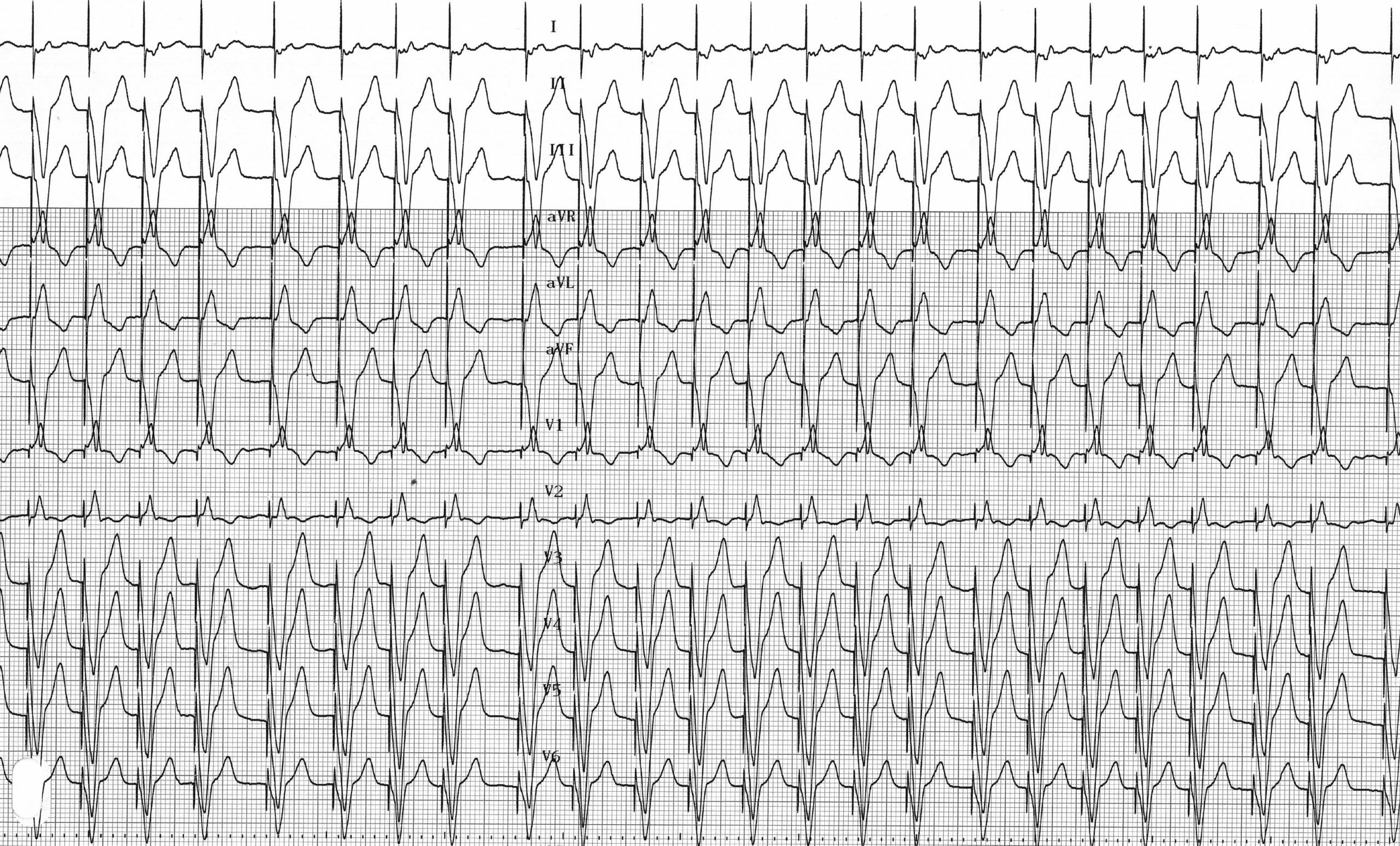
Electro-induced tachycardia; rapid and irregular ventricular pacing (which is inconsistent with a regular PMT); probable atrial fibrillation;
Explanation
The management of patients with pacemakers who experience episodes of atrial arrhythmia is complex due to the various known mechanisms that trigger atrial arrhythmias and the risk of ventricular pacing runaway upon detection of a rapid atrial rhythm.
The device can be programmed to respond to atrial arrhythmia by switching to an asynchronous mode to avoid high-frequency ventricular pacing that could compromise hemodynamic stability. Mode switching refers to the pacemaker’s ability to automatically switch from an atrial-led mode (DDD or VDD) to a non-atrial-led mode (DDI or VDI). The ventricular pacing rate gradually decreases from the maximum synchronous rate to the slave rate or base rate. This prevents a sudden drop in the ventricular rate. When the atrial tachyarrhythmia ends, mode switching returns to the programmed synchronous pacing mode.
Mode switching is programmed by default and must not be deprogrammed even if the patient has no known history of atrial arrhythmia. In this patient, the absence of a drop in rate is associated with prolonged rapid ventricular pacing at the maximum tracking rate. The combination of loss of atrial systole and runaway ventricular pacing is responsible for the observed signs of cardiac decompensation.
In this patient, it is necessary to program the retraction to prevent ventricular synchronization with rapid atrial activity.
Trace description
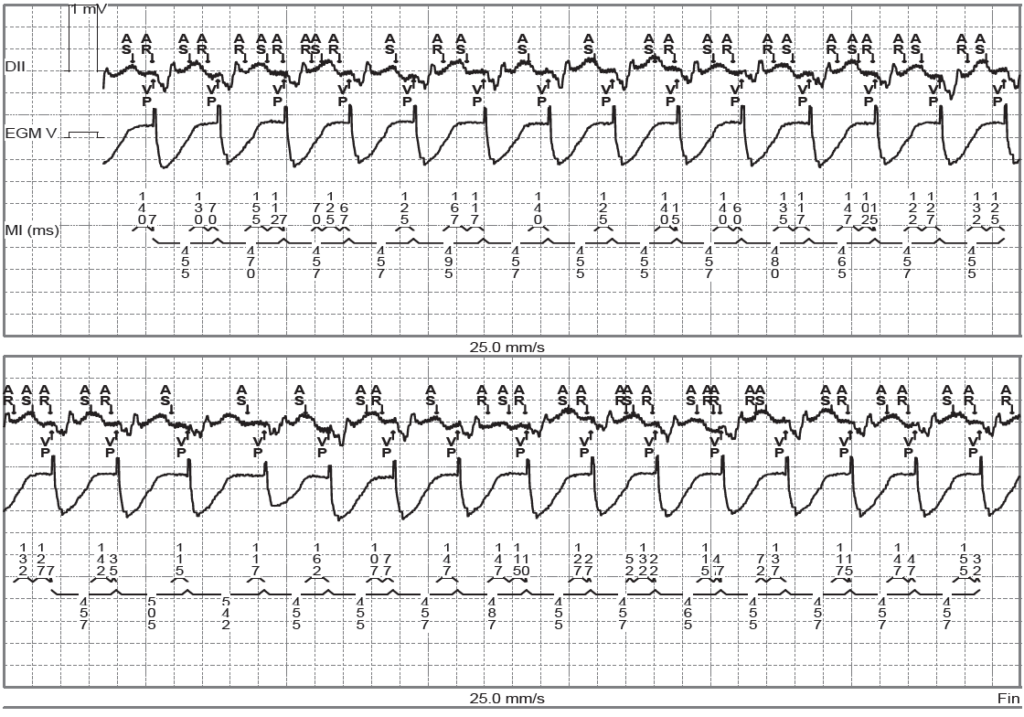
The EGM shows detection of a rapid, irregular atrial rhythm with continuous ventricular pacing; no recovery following detection of atrial fibrillation, which explains the rapid ventricular pacing;
To remember
An electro-induced ventricular tachycardia that is irregular and fluctuates around the maximum monitoring rate in a patient with a dual-chamber pacemaker should raise suspicion of atrial fibrillation and a deprogramming or malfunction of the fallback algorithm (mode switching).