

Trace description
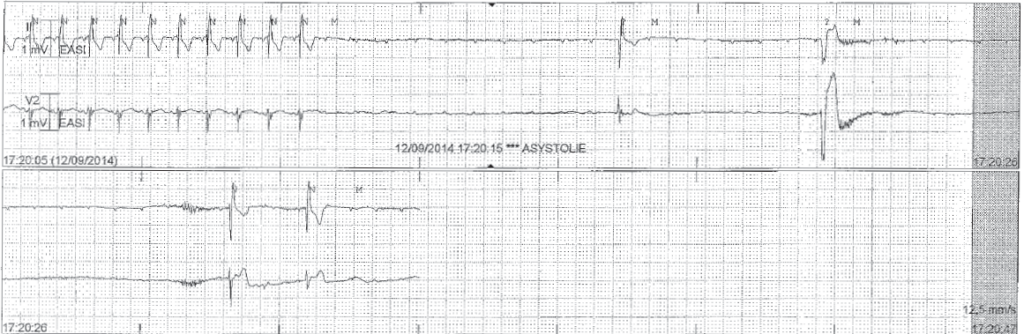
The patient is admitted with telemetry monitoring; new syncope episode with evidence on the tracing of a prolonged asystole with numerous blocked P waves; rare ventricular escape rhythms;
Commentary
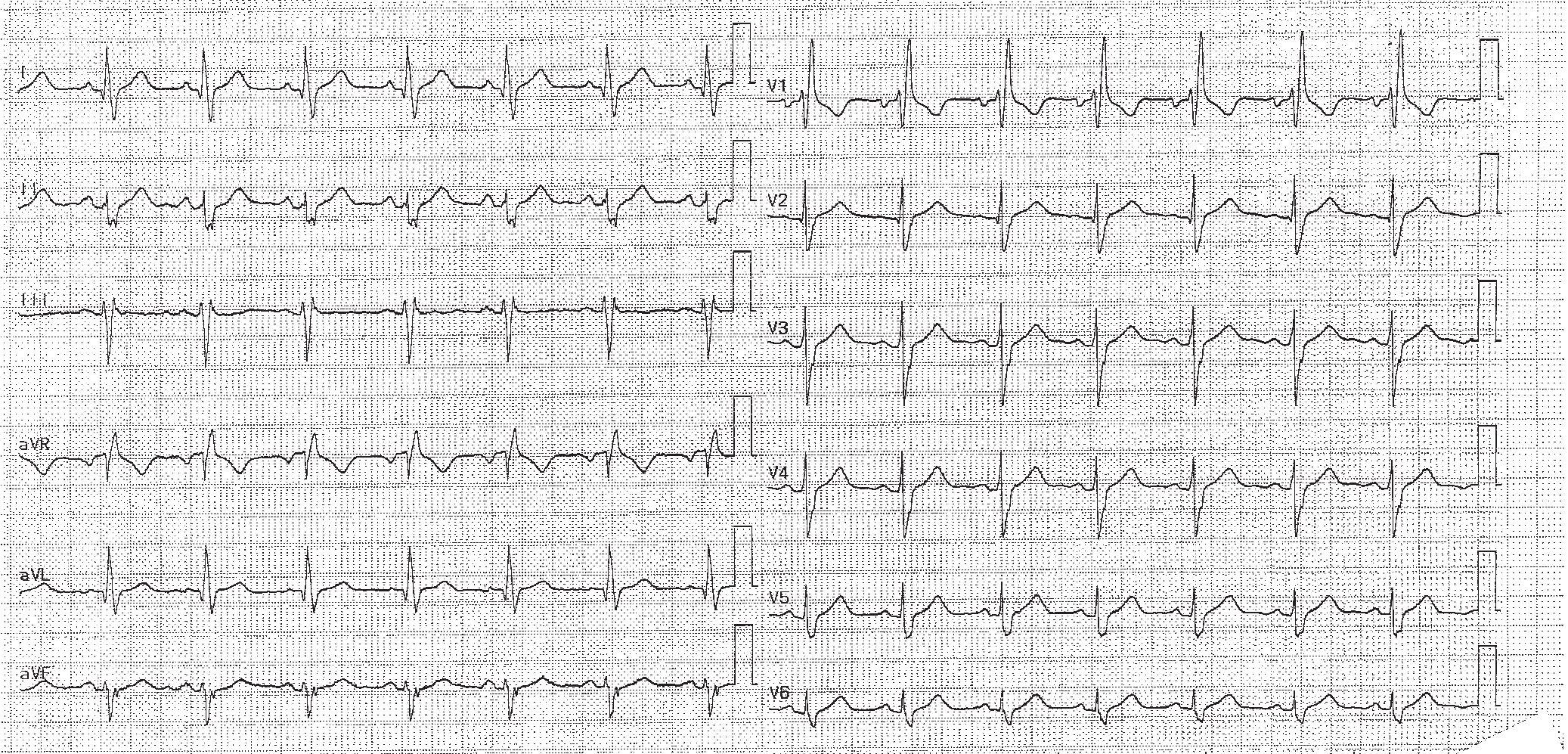
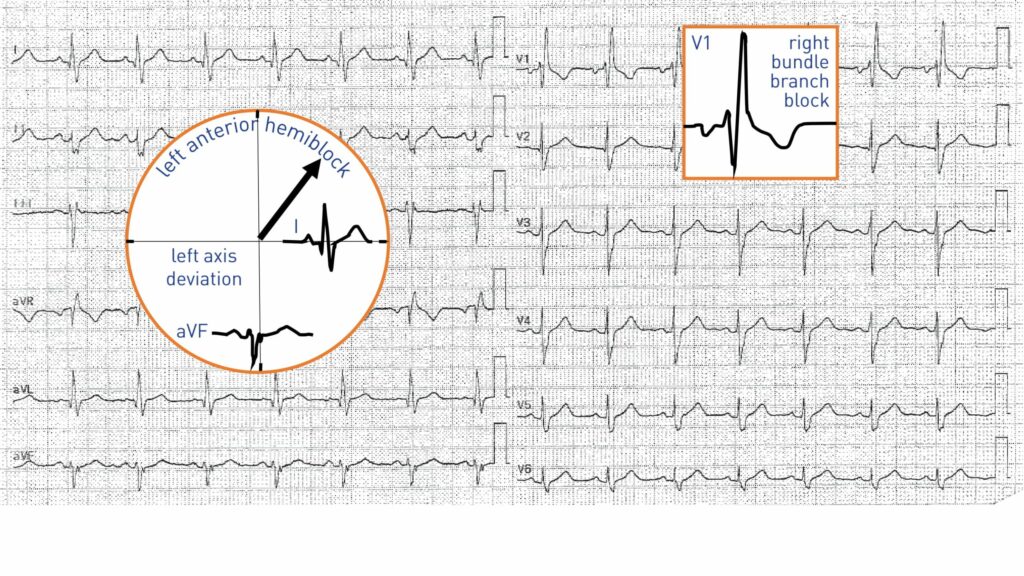
This patient initially presented a bifascicular block. The left axis deviation adding to a typical pattern of right bundle branch block should evoke the associated diagnosis of left anterior fascicular block.
This patient visited the emergency room following the occurrence of several syncopes within a brief time span (two days). Clinical (several convulsive syncopes with no obvious trigger) and electrocardiographic evaluation (conduction disorder) is strongly suggestive of a cardiac origin which justifies an immediate hospitalization with telemetry monitoring. The criteria for emergency hospitalization following syncope include (1) the presence of an underlying cardiac disease, (2) the presence of an electrocardiographic abnormality pointing to a conduction or rhythm disorder, 3) exertional syncope, 4) severe trauma, 5) family history of sudden death or inherited Brugada-type disease.
The association of right bundle branch block and left anterior fascicular block is relatively common. The fascicular block deviates the very first QRS vectors downward and to the right, the middle QRS vectors upward and to the left. The right bundle branch block adds terminal QRS vectors directed to the right (right ventricular potentials).

Trace description
A dual-chamber pacemaker is implanted; the electrocardiogram shows a rhythm predominantly detected in the atrium (a single paced atrial cycle) and paced in the ventricle (low right ventricular septal pacing lead explaining QRS negativity in lead I and in inferior leads); DDD pacing mode (synchronization of the ventricles on the paced or sensed atria);