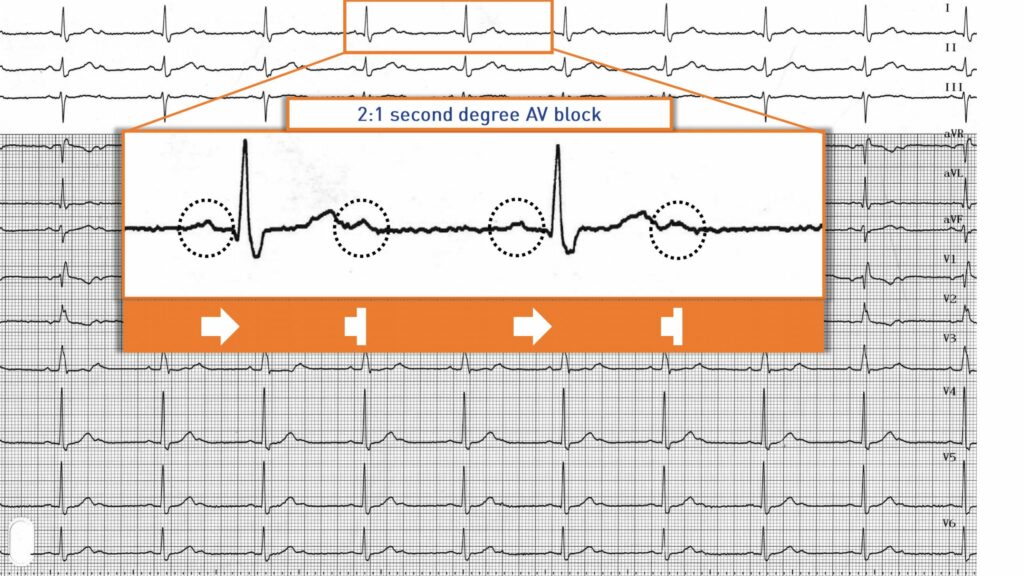
2-to-1 AV block deserves to be individualized as it is relatively common and represents a border zone between second-degree block and high-grade block since it comprises the same number of blocked waves as conducted P waves. It is difficult to determine the supra-, intra- or infra-Hisian location. The recording of long tracings may reveal a typical Wenckebach pattern with variations in the duration of the PR interval (in favor of a nodal Mobitz 1) or a Mobitz 2 pattern with several conducted P waves followed by a blocked P wave without modification of the PR interval (in favor of an intra- or infra-Hisian block).
In a 2:1 AV block, the PR interval of the conducted P waves is typically of normal duration but can be prolonged. Variations can be observed in the PP interval, with PP intervals with QRS complexes being shorter than PP intervals without QRS complexes (ventriculophasic sinus arrhythmia). Different hypotheses have been proposed to explain this alternation in atrial cycles (short PP cycle with QRS, long PP cycle without QRS): 1) ventricular depolarization could promote stretching of the right atrium responsible for an increase in automaticity of the sinus node and a decrease in PP interval; 2) ventricular depolarization is accompanied by an increase in cardiac output and an effect on baroreceptors, accompanied by a decrease in parasympathetic activation leading to an increase in the sinus rate.
In a high-grade block, non-conducting P waves are more numerous than conducted P waves. Atrioventricular conduction can occur at regular (3:1 block, 4:1 block, etc.) or irregular intervals. A junctional or ventricular escape beat is commonly observed causing a transient dissociative pattern with a few rare captures (conducted P waves).
In this symptomatic patient, the indication for pacemaker implantation is indisputable (class I indication).