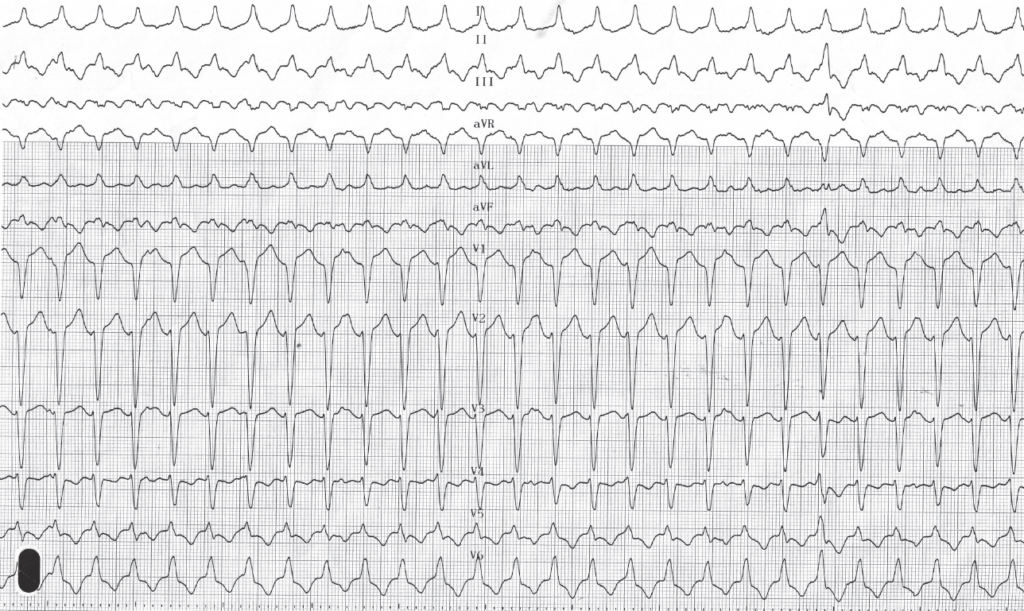
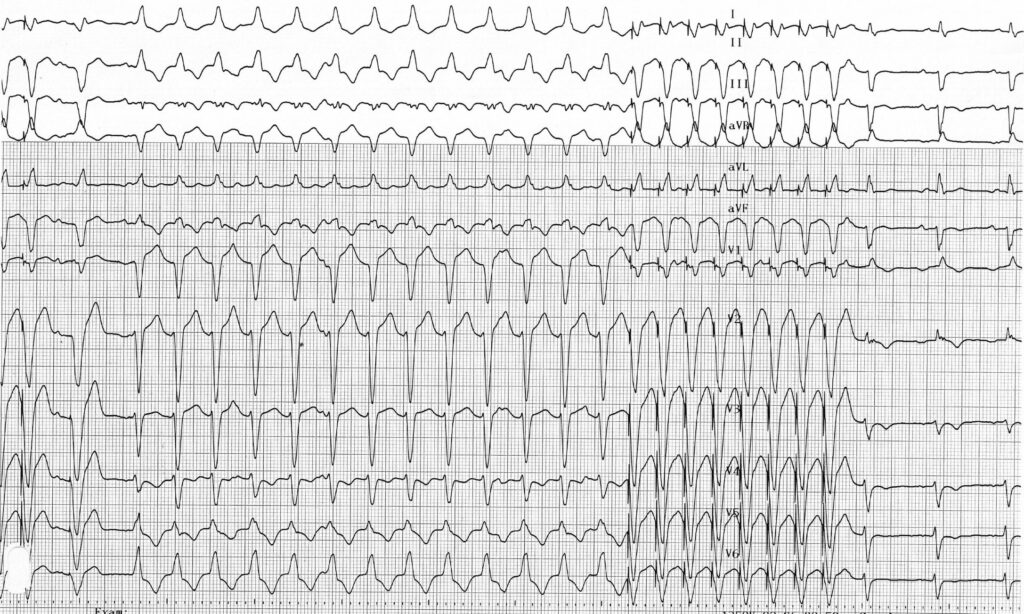
Trace description
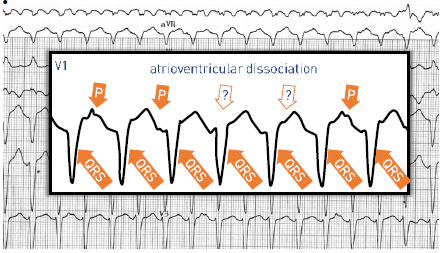
relatively slow ventricular tachycardia (130 bpm) with left delay; QRS transition (R/S>1) in V5 (late); atrioventricular dissociation confirming the diagnosis of ventricular tachycardia (atrial activity clearly identifiable in V1); this tracing corresponds to a right ventricular outflow tract (pulmonary infundibulum) tachycardia;
Commentary
arrhythmogenic right ventricular dysplasia is an inherited disease characterized by the gradual replacement of the cardiac muscle cells by fibro-adipose tissue. Transmission is autosomal dominant with variable penetrance and expression by mutation of the genes encoding for desmosome proteins. Dysplasia predominantly affects men with a male to female ratio of 3:1 and is usually manifested in young subjects, the symptoms appearing most often before the age of 40 years. The replacement of the myocardium with fatty tissue and fibrosis can be widespread and extend to the left ventricle in advanced forms or be more localized at the apex or right ventricular infundibulum. The evolution of the disease varies from one individual to another, with some patients remaining totally asymptomatic or presenting only minor symptoms. Histological abnormalities can contribute to the development of ventricular rhythm disorders that can lead to palpitations, syncope or sudden death due to intense sports activity. This disease is frequently found in high-level athletes having suffered a sudden death and is the second cause (after hypertrophic cardiomyopathy) of sudden death in the young patient. One of the difficulties in the management of these patients is that the first observed clinical manifestation may be the occurrence of sudden death. When the disease evolves, symptoms related to a right and subsequently biventricular heart failure may appear.
Diagnosis is based on the detection of a combination of major as well as minor clinical, ECG or morphological criteria. The aim of the evaluation is to confirm the diagnosis, to assess the risk of sudden death and to specify the extent of the disease.
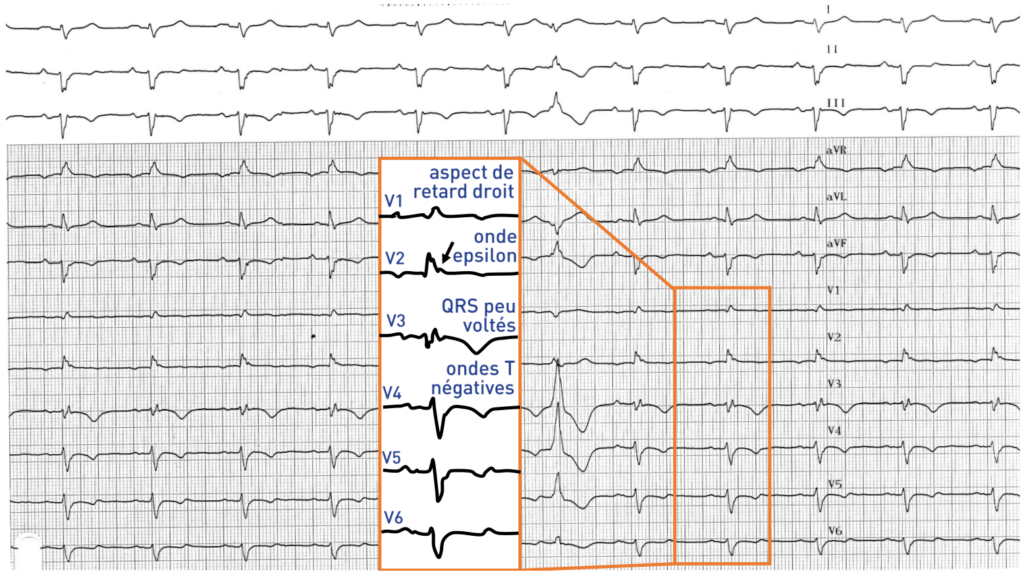
The surface electrocardiogram plays a central role since some criteria are considered as major others as minor. It can reveal:
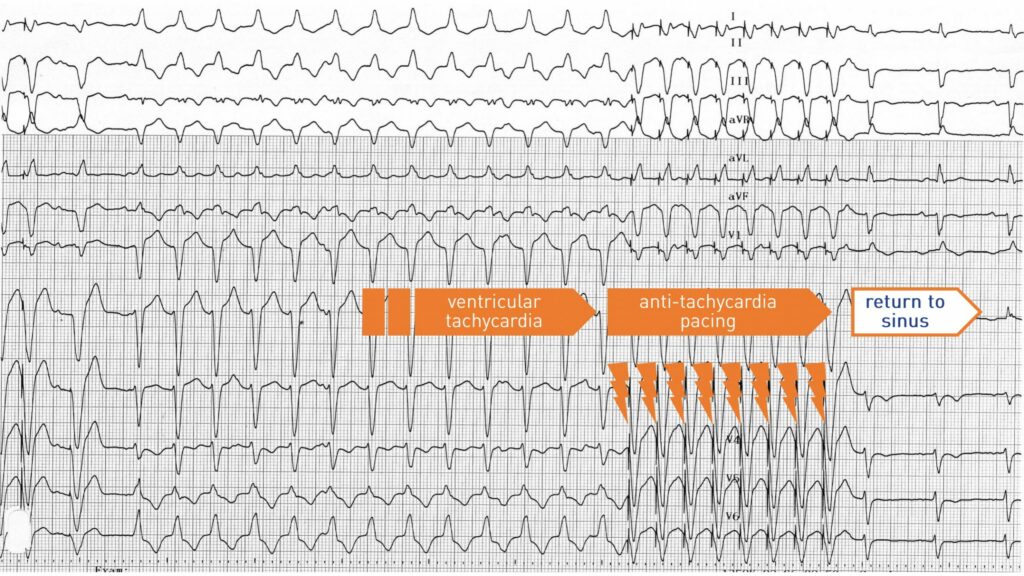
Trace description
This tracing shows an anti-tachycardia pacing sequence delivered by the implantable defibrillator which allows the interruption of the tachycardia and the return to sinus rhythm;
Commentary
In addition to the electrocardiogram, several supplementary exams are performed:
Therapeutic management varies according to the severity of the disease. Severe cardiac arrhythmias occurring most often upon physical exertion, competitive sports are contraindicated. High dose beta-blockers are the reference medical treatment. Radiofrequency ablation can be proposed essentially in patients with episodes of recurrent ventricular tachycardia resistant to medical treatment. Patients most at risk of sudden death must undergo implantation of a defibrillator. Recognized risk factors are recovered sudden death, syncope, history of familial sudden death or recurring rhythm disorders despite well-monitored medical treatment.