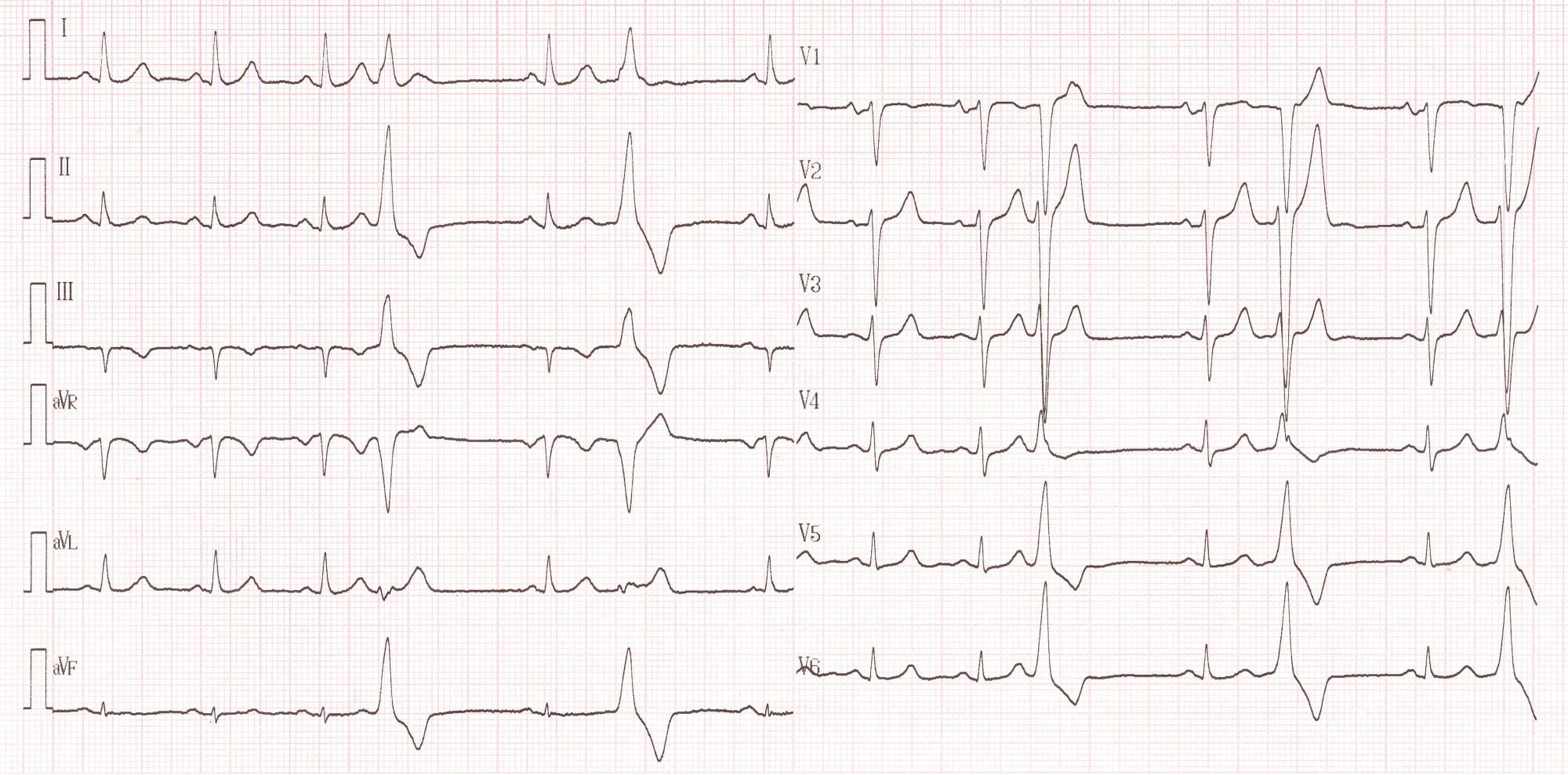
42-year-old man followed by his cardiologist for evidence of ventricular extrasystoles; sensations of palpitations occurring during recovery after physical exertion;
ECG description
A complete assessment is performed (cardiac ultrasound, ventricular late potentials, exercise test, MRI) without any detected abnormality; an isoproterenol test is performed: during recovery, sinus tachycardia followed by tachycardia of 200 bpm with a morphology identical to extrasystoles; clinical reproduction of symptomatology experienced by the patient at the time of palpitations; preserved hemodynamics and spontaneous termination after 20 seconds of tachycardia;
Explication
This patient hence presented episodes of right infundibular ventricular tachycardia. This type of tachycardia is considered to be benign and classically observed in young patients, aged 20 to 40 years on average, devoid of heart disease, without male or female predominance. The clinical presentation varies with perfectly asymptomatic patients or the description of palpitations, lipothymias and more rarely syncope. Two types of distribution of the arrhythmias have been described, both with a generally favorable clinical course: unsupported but incessant episodes, or sustained, paroxysmal and recurrent episodes. An adrenergic feature upon the occurrence of arrhythmias has been found in some patients, the majority of episodes occurring during or just after physical exertion. Stress, caffeine or certain phases of the menstrual cycle in women can also promote its occurrence. Infundibular ventricular tachycardia is usually well tolerated since occurring in patients without cardiomyopathy. The description of certain isolated cases of sudden death could call into question its alleged benign nature, but must above all warrant reconsideration in this setting of a differential diagnosis such as right ventricular dysplasia.
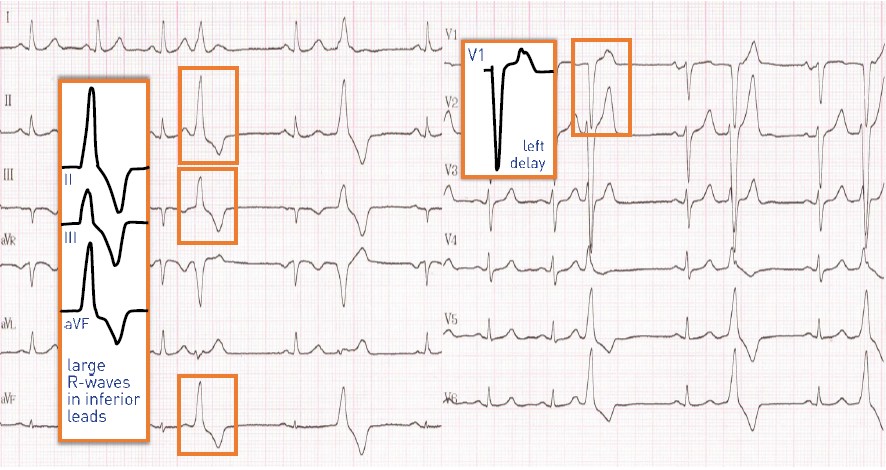
Benign infundibular tachycardias display certain electrocardiographic characteristics:
• left delay and inferior axis;
• atrial activity is often dissociated even though there may be a 1:1 retrograde conduction;
• QRS duration is generally only moderately increased (1 pattern) occurs in V3 or V4 whereas it often occurs earlier when it originates from the left ventricle outflow tract or from a coronary cusp; while most of these tachycardias have a left delay, there are some described cases of right delay, its left ventricular origin being no longer in doubt;
• aside from the tachycardia, the electrocardiogram is most often normal although approximately 10% of these patients present a complete or incomplete right bundle branch block; in the context of the differential diagnosis, it is important to investigate for signs evocative of arrhythmogenic right ventricular dysplasia (negative T waves in V1-V3, epsilon wave, polymorphism of extrasystoles, etc.);
The diagnosis of idiopathic ventricular tachycardia in a healthy heart should be given after elimination of certain diseases. As explained above, in the case of ventricular tachycardia with left delay, the main differential diagnosis is arrhythmogenic right ventricular dysplasia: the evaluation therefore involves the performing of late potentials (most often negative), a cardiac ultrasound (absence of heart disease), a normal BNP measurement, an isoproterenol test which can favor the occurrence of arrhythmias but with no identified polymorphism (multiple morphologies). The performing of an MRI currently represents the reference examination to exclude the diagnosis of dysplasia since it allows a detailed morphological and dynamic analysis of the right ventricle.
Commentary
Unlike a large number of ventricular tachycardias (post-infarction, fascicular, dysplasia, etc.), the mechanism involved in this arrhythmia is not a reentry but a triggered activity sensitive to cAMP in conjunction with late post-potentials (oscillation of the membrane potential during phase 4 of the action potential). The occurrence of these triggered activities is favored by the elevation in intracellular calcium concentration or by a catecholamine discharge. At the cellular level, the elevation of plasma cAMP concentration is the determining factor, which will have a significant impact on the therapeutic treatments to be proposed. Any situation that increases the intracellular concentration of cAMP has a proarrhythmic effect (isoproterenol, for example). In contrast, any situation that causes a decrease has an antiarrhythmic effect (beta-blockers, verapamil).
The decision to treat should integrate the presence of symptoms and their severity, the prognosis of these patients being a priori not altered. The long-term effectiveness of beta-blockers or verapamil is modest. When medical treatment is minimally effective or poorly supported, radiofrequency ablation amy be proposed. Induction of tachycardia is more often performed by injection of isoproterenol than by programmed ventricular pacing (it is not a reentry). The success rate is high and the rate of recurrence and complications is limited.
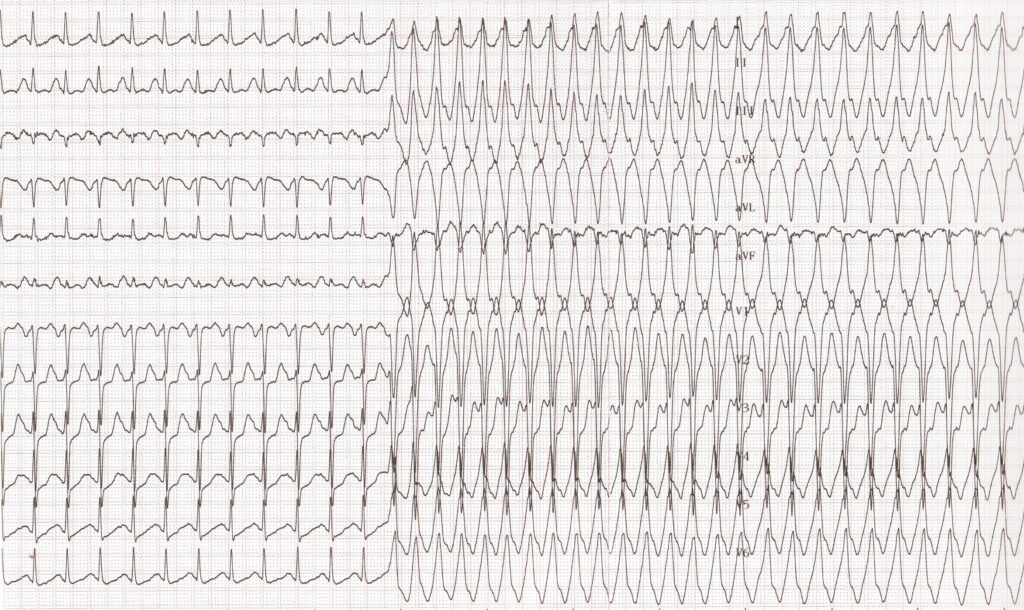
Trace description
A complete assessment is performed (cardiac ultrasound, ventricular late potentials, exercise test, MRI) without any detected abnormality; an isoproterenol test is performed: during recovery, sinus tachycardia followed by tachycardia of 200 bpm with a morphology identical to extrasystoles; clinical reproduction of symptomatology experienced by the patient at the time of palpitations; preserved hemodynamics and spontaneous termination after 20 seconds of tachycardia;
To remember
Right ventricular outflow tract ventricular tachycardia occurs preferentially in a young patient without heart disease with a characteristic electrocardiographic pattern: monomorphic tachycardia, slightly widened QRS, left delay and inferior axis, atrioventricular dissociation. A late precordial transition (R/S > 1) (in leads V3, V4 or V5) is suggestive of RV outflow tract origin