Trace 8.10: Ischemic ventricular fibrillation
Patient information
61-year-old man with risk factors (active smoking and dyslipidemia) admitted to the intensive care unit for an acute anterior coronary syndrome; angioplasty was performed with stent placement in the anterior interventricular coronary artery 12 hours after the onset of symptoms; severely diminished left ventricular ejection fraction (30%); 10 days after this episode, new hospitalization for a recovered sudden death;
ECG
Question
What is(are) the possible diagnosis(es) on this ECG?
Commentaires
ECG description
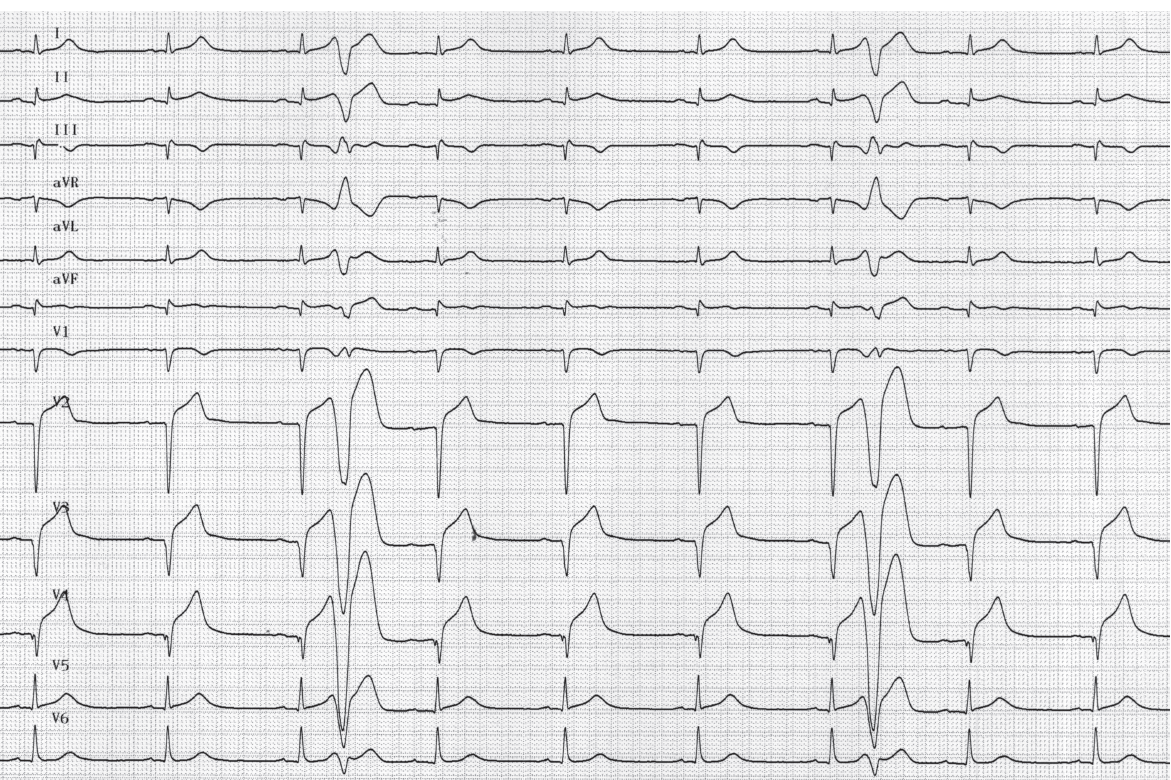
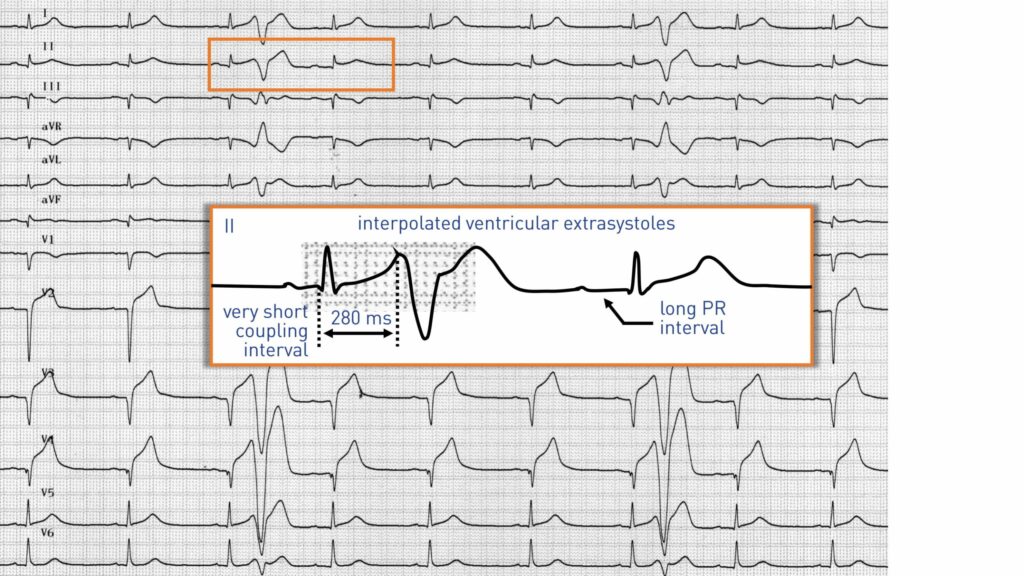
Sinus rhythm; signs of prior extensive anterior infarction (Q wave from V1 to V4 and in inferior leads); persistence of ST segment elevation indicating incomplete or late reperfusion; two interpolated ventricular extrasystoles (no variation in sinus rhythm) with very short coupling interval (coupling of 280 ms); these extrasystoles originate in the left ventricular septoapical wall; the ensuing P waves are conducted with a long PR interval (hidden conduction of the extrasystole);
Explication
The causes of sudden death in the aftermath of a myocardial infarction are multifactorial and vary according to the delay relative to the onset of symptoms. An ischemia-induced ventricular fibrillation is responsible for most deaths occurring during the pre-hospital phase. The incidence then decreases regularly although the risk remains present particularly when the infarction is extensive and reperfused late. Episodes of ventricular fibrillation may also occur at the late stage of hospitalization in patients with extensive necrosis and primarily affecting the anterior area. An extended telemetry monitoring is therefore desirable in patients having extensive necrosis with late reperfusion, especially since there are frequent, premature and polymorphic ventricular extrasystoles. The onset of a ventricular fibrillation most often occurs on a succession of short cycle (ventricular extrasystole)-long cycle (compensating pause)-short cycle (new extrasystole). This patient presented multiple episodes of ventricular fibrillation a few days after an episode of extensive late-reperfused myocardial infarction in spite of beta-blocker treatment and temporary sedation. A control coronary angiography showed no intra-stent restenosis. An ablation procedure was performed with evidence of a Purkinje potential in the middle of the scar. Arrhythmia episodes were triggered by the occurrence of ventricular extrasystoles originating from the Purkinje fibers which had survived under anaerobic conditions. The ablation procedure allows recovering a highly compromised situation with iterative episodes of polymorphic ventricular arrhythmias that quasi-systematically led to death. In this setting, the major role of the Purkinje system and of cells located in the border zone has been demonstrated and validated by the decrease or disappearance of arrhythmias after localized ablation.

Trace description
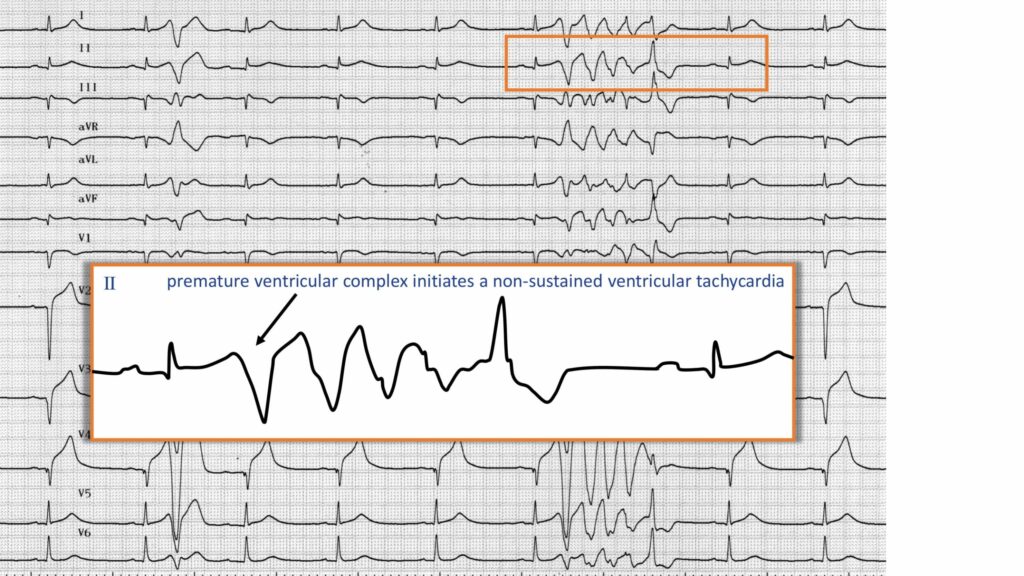
Identical morphology of the ventricular extrasystole; extrasystole triggering a burst of nonsustained polymorphic ventricular tachycardia;

Trace description
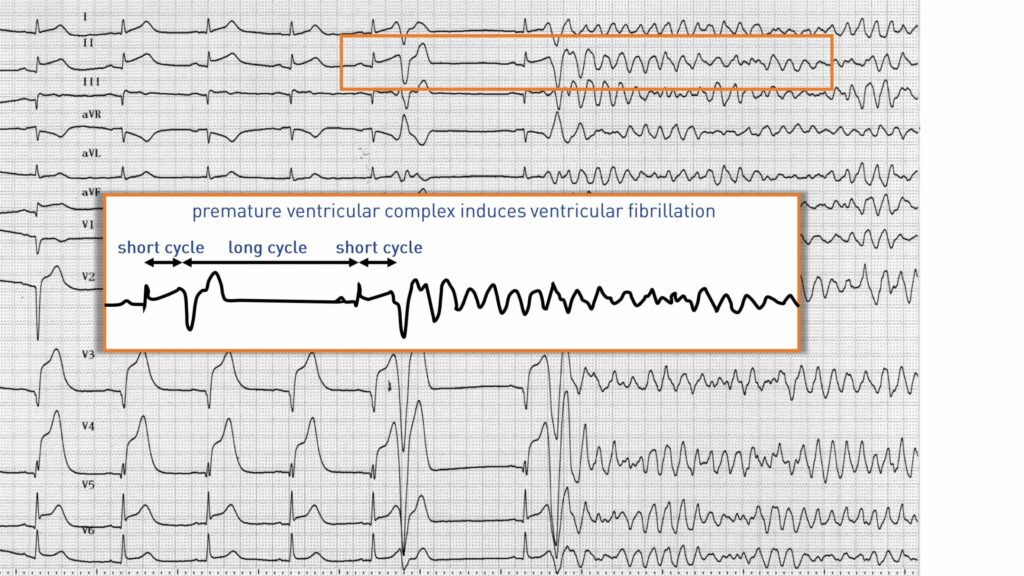
Ventricular extrasystole with a slightly different morphology; retrograde atrial conduction and compensatory pause after the extrasystole; second ventricular extrasystole inducing an episode of ventricular fibrillation (wide QRS tachycardia, irregular, polymorphous, disorganized, tall oscillations with loss of alternation between systoles and diastoles); sudden onset of the arrhythmia after a ventricular extrasystole and a short cycle-long cycle-short cycle sequence; an electric shock was necessary to restore sinus rhythm;
To remember
In the aftermath of myocardial scar, the survival of Purkinje fibers under anaerobic conditions may contribute to the occurrence of ventricular fibrillation and sudden death.