Trace 7.10: Wolff–parkinson–white and AV-block
Patient information
79-year-old man with no known history or intimation of palpitations, hospitalized for multiple lipothymia episodes;
ECG
Question
What is(are) the possible diagnosis(es) on this ECG?
Commentaires
ECG description
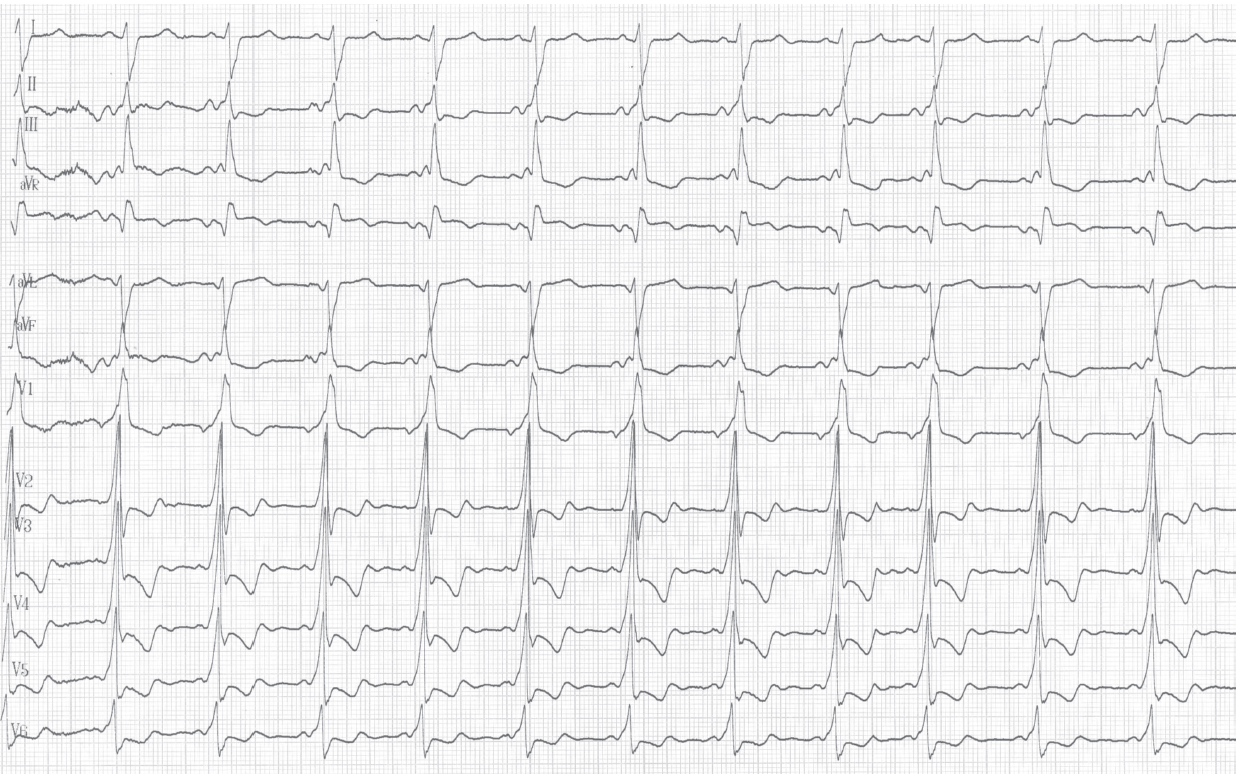
This first tracing performed on arrival in the emergency department shows a typical tracing of left lateral accessory pathway (short PR and delta wave) with a major pre-excitation pattern and a very broad QRS;
Explication
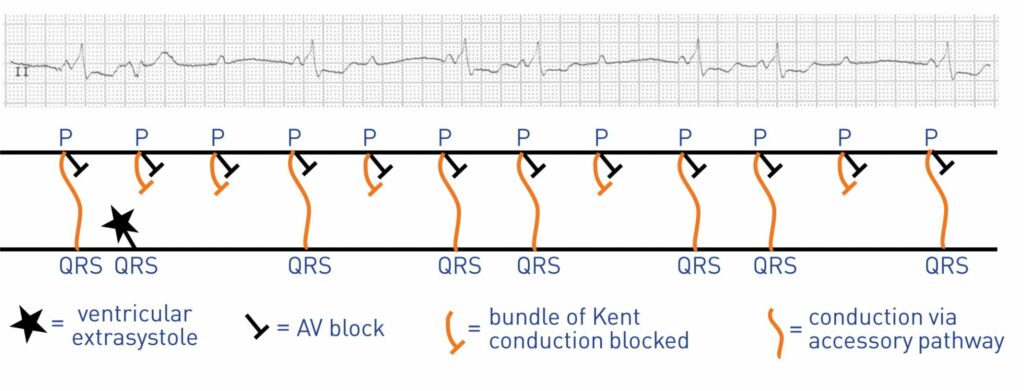
In a patient with Wolff-Parkinson-White syndrome, sinus rhythm is usually conducted to the ventricles through two different pathways; the atrioventricular node and the bundle of Kent, the QRS reflects fusion of these two activations. The present case shows a rare case of complete atrioventricular block on the Hisian pathway associated with a second degree block on the accessory pathway. The anterograde conduction is therefore interrupted in a paroxysmal manner leading to the occurrence of dizzy-spells. The complete atrioventricular block could already be suspected given the completely preexcited pattern on the first tracing, which is a rare occurrence in the context of a left lateral accessory pathway. Patients with Wolff-Parkinson-White syndrome complain much more of palpitations and episodes of tachycardia than of issues related to bradycardia. Indeed, the accessory pathway normally has a protective effect during the occurrence of a conduction block on the nodo-Hisian pathway. In the presence of a syncopal episode, the occurrence of a rapid tachycardia (orthodromic, antidromic or atrial fibrillation) is generally suspected. In this patient, a conduction disorder occurring on both pathways was responsible for the described symptoms. A dual-chamber pacemaker was implanted and remotely-conducted controls showed a high percentage of ventricular pacing indicating the presence of a permanent conduction disorder.
Trace description
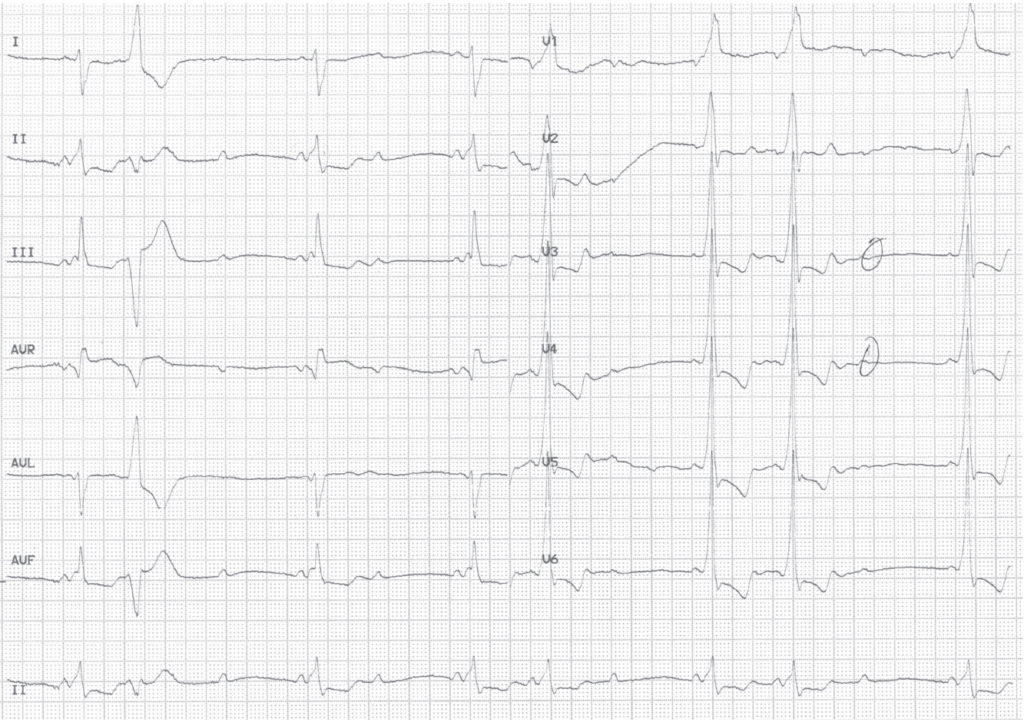
On this second tracing, there are blocked sinus P waves and P waves followed by a pre-excited ventricle identical to those of the previous tracing; this tracing suggests the presence of a complete block of the normal atrioventricular conduction pathways explaining the maximum pre-excitation pattern (exclusive conduction by the accessory pathway) and a second degree block in the bundle of Kent (alternation between conducted P waves and blocked P waves);
To remember
A patient with an anterograde permeable accessory pathway exhibits a fully preexcited pattern (maximum pre-excitation) following the occurrence of a conduction block on the nodo-Hisian pathway. The accessory pathway typically has a protective effect in this setting.