Trace 7.1: Accessory pathway, bundle of Kent, wolff-parkinson-white syndrome
Patient information
young man 21 years of age applying for a professional firefighter’s position, referred for identification of an abnormal tracing; presented some episodes of tachycardia with sudden onset and end;
ECG
Question
What is(are) the possible diagnosis(es) on this ECG?
Commentaires
ECG description
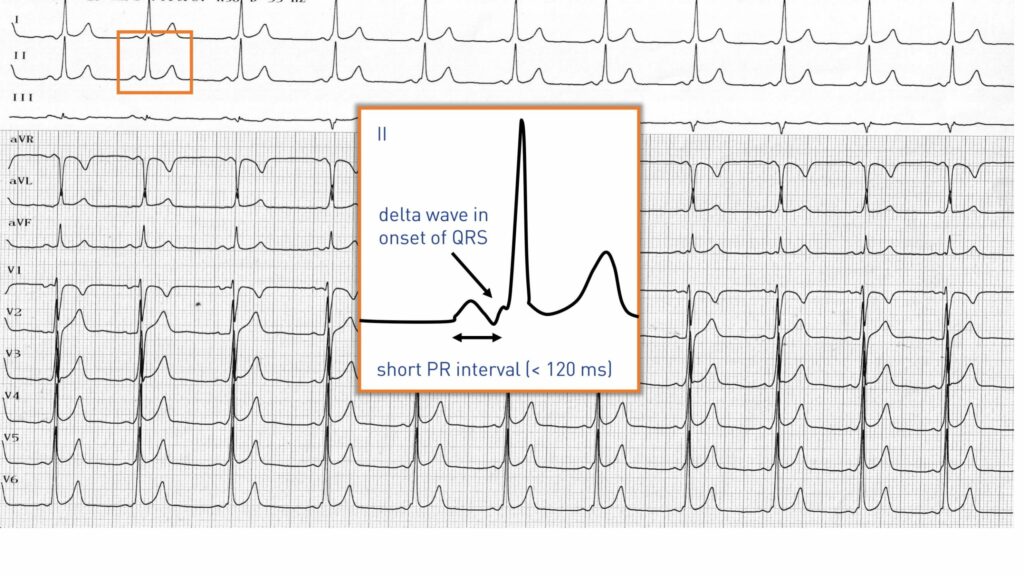
This electrocardiogram shows a typical pattern of ventricular pre-excitation: short PR interval (< 120 ms), delta wave at the beginning of the QRS, non-prolonged PJ delay, terminal QRS portion without abnormality;
Explication
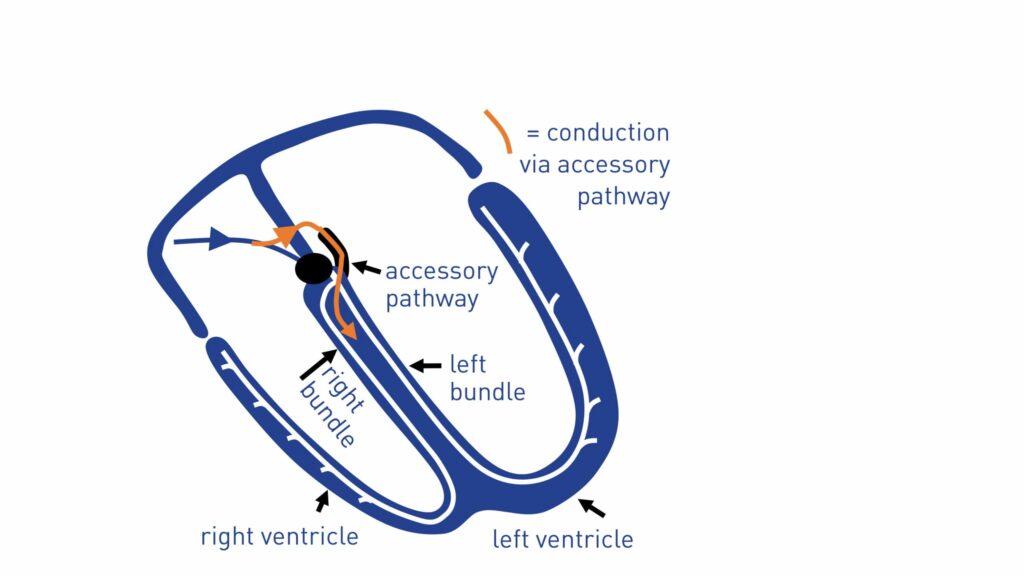
This young patient has an accessory pathway with intermittent anterograde conduction. Conduction in an accessory pathway operates on the all-or-nothing principle: the bundle is either in a refractory period or not, and the impulse is or is not transmitted to the ventricles. The anterograde refractory period of this pathway is long, a slow atrial activity is thus necessary for the pre-excitation to become visible. During higher rate, the electrocardiogram is normal (phase 3 block). This type of accessory pathway is considered benign as a long refractory period protects the patient from the risk of sudden death secondary to rapid atrial fibrillation conducted by the pathway. On the other hand, this particular pattern is associated with a short retrograde refractory period of the pathway and this patient presented with orthodromic reentry tachycardia (good retrograde conduction) with a disabling symptomatology. Given the frequency of the seizures (daily tachycardias), the patient underwent the ablation of an anteroseptal pathway.
Commentary
Anterograde conduction is sometimes present but difficult to visualize (concealed Kent). For a left lateral pathway, the time required for the impulse to travel from the sinus node to the left atrium is longer than the transit time toward the nodo-Hisian pathway explaining the presence of a minimal delta wave. The absence of a septal q wave in leads V5-V6 should evoke an accessory pathway in a patient with palpitations. While the presence of a hidden accessory pathway (no anterograde conduction) does not expose the patient to the risk of sudden death due to rapid atrial fibrillation, this is not the case for a concealed accessory pathway; indeed, the difficulty in visualizing the accessory pathway is due to a significant distance between the sinus node and the pathway but not to a long refractory period.
Trace description
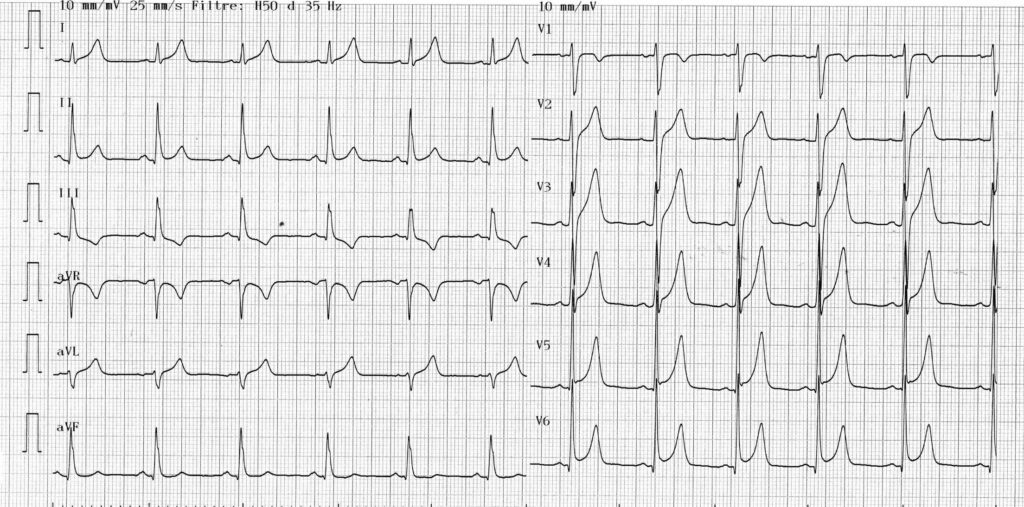
this young patient underwent ablation of a left posteroseptal accessory pathway; the PR interval is normalized with disappearance of the delta wave (more pronounced slowing of the beginning of the QRS) and appearance of a physiological septal q wave in V5-V6; early repolarization pattern that could potentially normalize remotely to the ablation;
To remember
the Wolff-Parkinson-White syndrome is defined by the combination of an atrioventricular pre-excitation (bundle of Kent) and paroxysmal supraventricular tachycardias. The diagnosis of atrioventricular pre-excitation in sinus rhythm is established on the association between a short PR interval, a wide QRS, a delta wave, a normal terminal QRS portion and frequent repolarization disorders.


