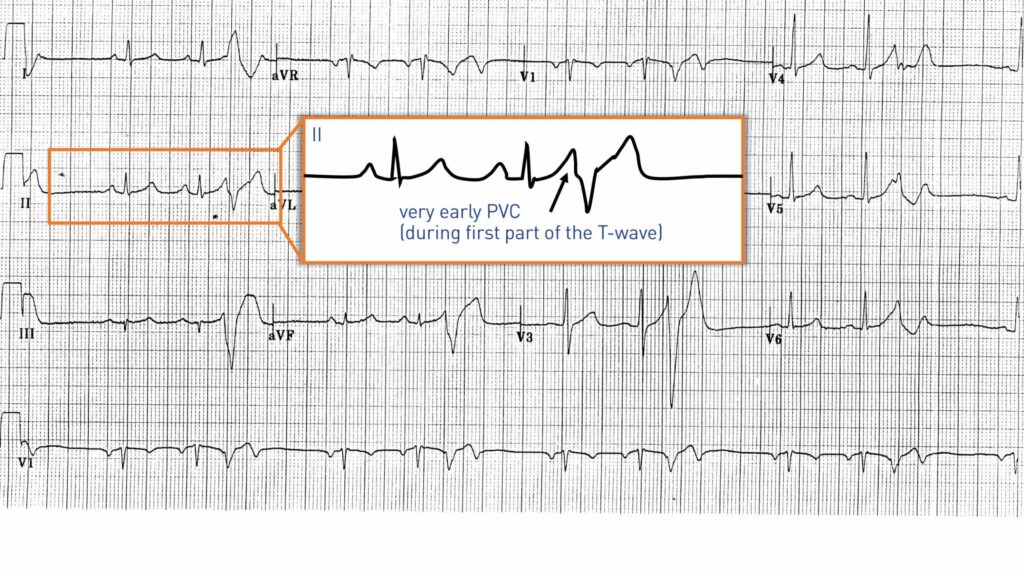
The presence of a short coupling interval between the premature ventricular complex and the preceding QRS complex represents a major risk factor for the development of ventricular arrhythmia. The premature ventricular complexes, when occurring in the ascending phase or at the peak of the T wave (R-on-T phenomenon), the ventricular vulnerable phase, are considered to be of short coupling interval and may favor the initiation of a malignant ventricular arrhythmia (short-coupled torsade de pointes or ventricular fibrillation). The triggering mechanisms of fibrillation at the atria and fibrillation at ventricles are probably very similar with interaction between a triggering factor and a substrate. The importance of the Purkinje network in the initiation of certain episodes of ventricular fibrillation has recently been suggested. The differentiated fibers of the Purkinje network can survive after the occurrence of a transmural infarction and develop arrhythmogenic electrophysiological properties. As is the case of pulmonary veins in focal atrial fibrillation, the Purkinje network can be the source of the initiating trigger of ventricular arrhythmia and can also promote its maintenance.
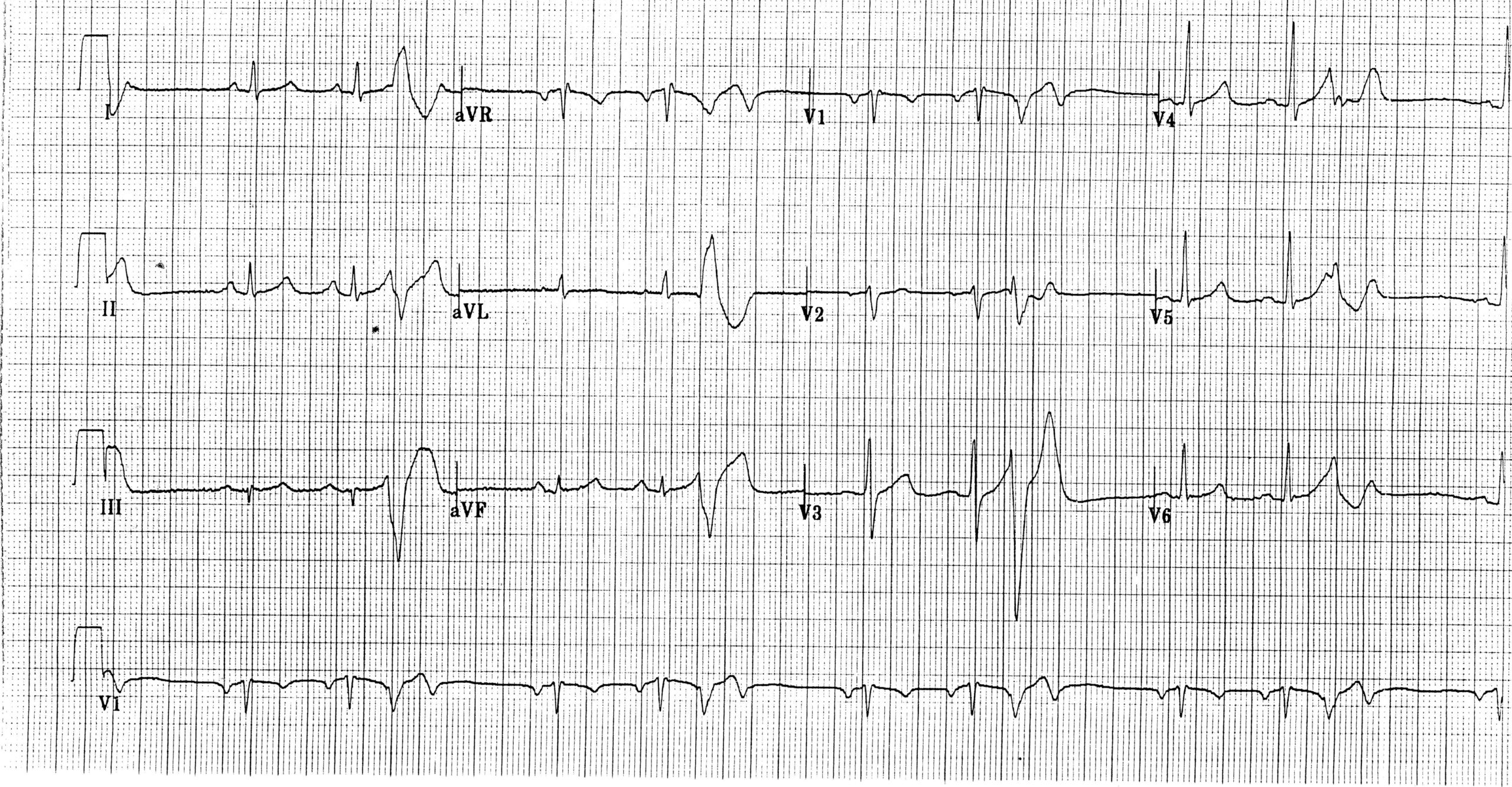
The pattern found on this tracing corresponds to a premature ventricular complex originating from the distal right ventricular Purkinje network: the complexes are very premature, relatively wide with a left delay. Premature complexes from the right ventricular Purkinje network, as in this patient, are most often monomorphic with a left delay, upper axis pattern and have an average duration of approximately about 140 ms. Those originating from the left ventricular Purkinje network are usually polymorphic, and are also very premature with a characteristic narrower QRS (120 ms on average).
This very particular type of premature complexes (very short coupling interval) is an undeniable marker of severity which should prompt an extensive investigation of the patient, as long as there is a notion of lipothymia/syncope or a family history of sudden death. Radiofrequency ablation of these premature ventricular complexes allows a cure in the majority of cases, the implantable defibrillator remaining indicated in secondary prevention.