A premature ventricular complex corresponds to premature excitation from the ventricular myocardium or ventricular conduction tissue from a point below the bifurcation of the right and left bundle branches. The prevalence of premature ventricular complexes is approximately 3% when performing a single ECG, whereas it can reach 50% in healthy subjects in instances of continuous recording over several days. The management of premature ventricular complexes constitutes a frequent reason for consultation, the setting of its discovery being highly variable: simple screening examination during the conducting of an ECG in an asymptomatic patient within the framework of a medical check-up for a sports fitness certificate, or check-up for palpitations, syncope or recovered sudden death. Premature ventricular complexes should preferentially be considered as a risk marker which should guide the search for a heart disease and not as an independent risk factor on which to act. The search for a causal heart disease is hence an essential component of management.
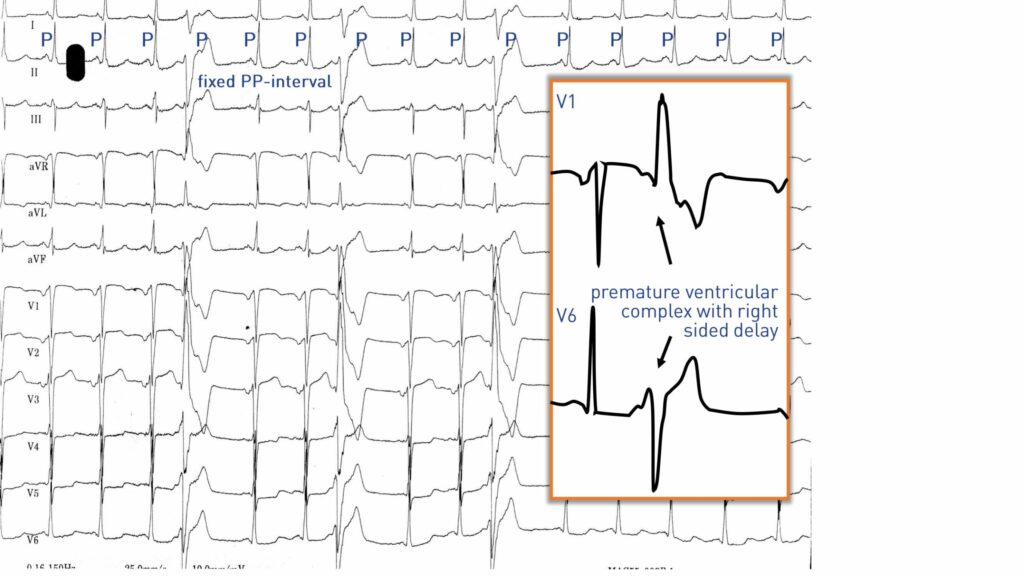
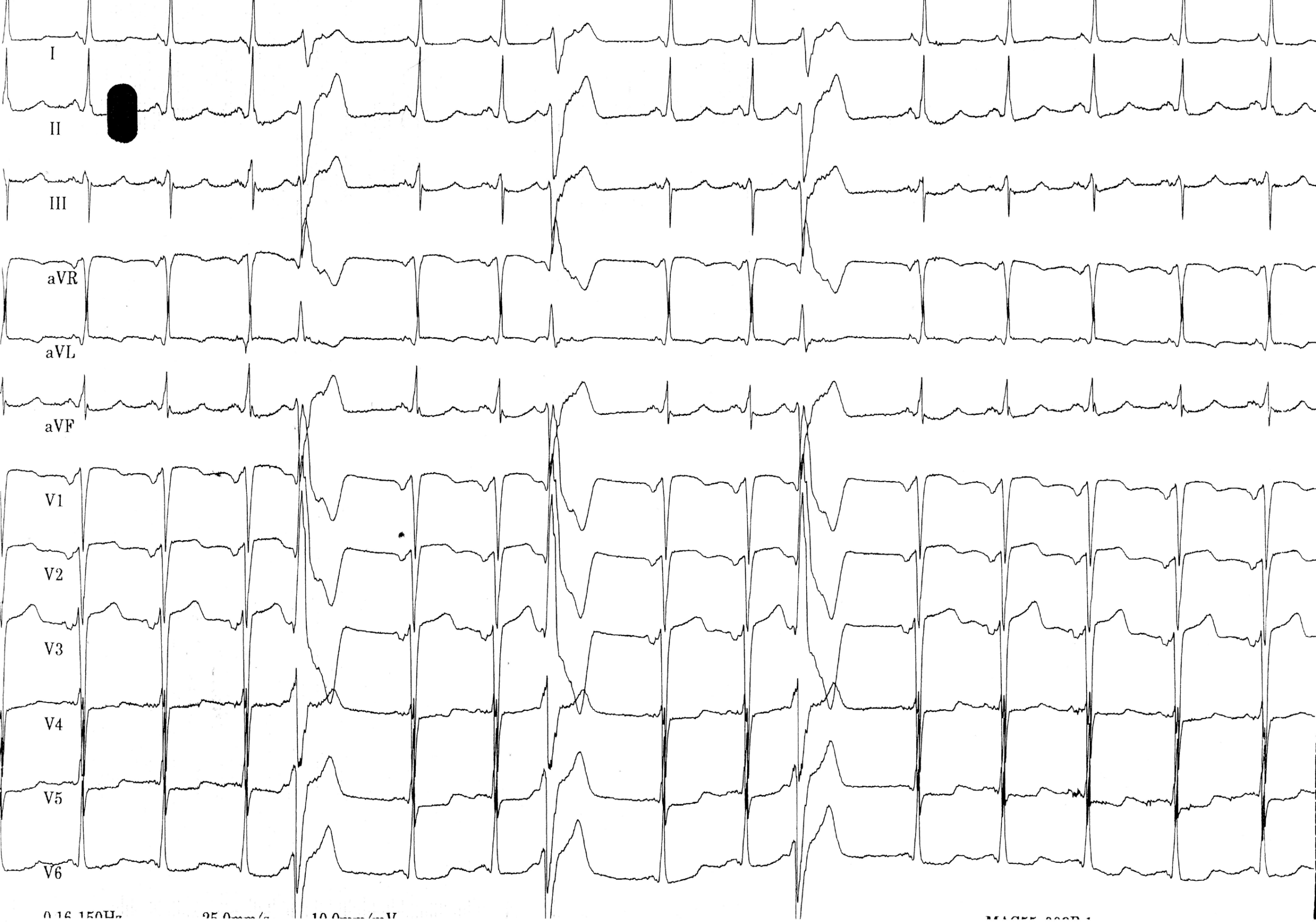
On the electrocardiogram, a premature ventricular complex is characterized by the presence of an ectopic, premature QRS, with broad QRS (> 120 ms), without association with a preceding atrial activity.
In this patient:
1. the analysis of the conducted QRS based on a sinus activity (P wave) is very much in favor of the presence of an ischemic heart disease. There are indeed signs of left atrial enlargement but also signs of a prior anterior infraction confirmed by anamnesis and analysis of the patient’s prior history;
2. the morphology of the premature complexes also points to the presence of heart disease. The width of the ectopic QRS complexes is significant and exceeds 180 ms, which is evocative of heart disease, given that the benign premature ventricular complexes occurring in a healthy heart are generally much narrower (of the order of 140 ms). The extrasystoles have a notched, polyphasic pattern with a relatively small amplitude, which also argues against a benign nature. The fragmentation of extrasystoles is considered a pejorative factor, since reflecting a propagation of electrical impulses through a ventricular myocardium with altered conduction properties, or in a scarred or fibrotic myocardium. In patients with ischemic cardiomyopathy, the delay and axis of the premature complexes are often dictated by the localization of the sequela of necrosis since these premature ventricular complexes are either the reflection of an abnormal activity of cells whose functioning is altered by the ischemia or the result of a reentry around slow-conducting pathways within the scar areas.