

Pacemaker mediated tachycardia (PMT) is the term used to describe an electrically driven tachycardia that most often occurs at the maximum pacing rate, with repeated sequences of ventricular pacing followed by retrograde atrial conduction. The initiation of a PMT results from the detection, outside refractory periods, of a retrograde P’ wave, which triggers an AV delay—often prolonged—that in turn promotes retrograde conduction following ventricular pacing. A PMT is therefore a repetitive sequence in which the pacemaker responds to each retrograde P’ wave by pacing the ventricle at a high rate, which in turn generates a retrograde P’ wave. The cycle thus repeats indefinitely unless a retrograde block occurs or a specific pacemaker algorithm intervenes.
The presence of retrograde conduction is therefore an essential prerequisite for initiating and maintaining a PMT. Retrograde conduction is present in an average of 40% of patients receiving pacing at rest, across all indications. It is much more common in patients implanted for sinus node dysfunction than for atrioventricular block. These figures are high enough to warrant the systematic programming of effective protection. In addition to the presence of retrograde conduction, initiating a PMT requires programming an atrial pacing mode (DDD or VDD) and results in a temporary or permanent loss of atrioventricular synchronization. Indeed, if ventricular activity is properly synchronized with that of the atrium, retrograde conduction is blocked. The following events can promote temporary atrioventricular dissociation, retrograde conduction, and the triggering of a PMT: a ventricular extrasystole (the most common cause), an atrial premature beat with prolongation of the AV delay to maintain the programmed maximum heart rate, a programmed AV delay that is too long (the atrioventricular bundle has emerged from its refractory period at the time of ventricular pacing), external interference or myopotentials detected by the atrial lead, a failure in atrial detection or pacing…
Early pacemakers were not protected against this type of runaway activity, and tachycardia could persist indefinitely, causing symptoms that were sometimes highly debilitating. Prolonged PMT can indeed be difficult to tolerate, with symptoms ranging from a simple feeling of discomfort or palpitations to cardiac decompensation in patients with underlying heart disease.
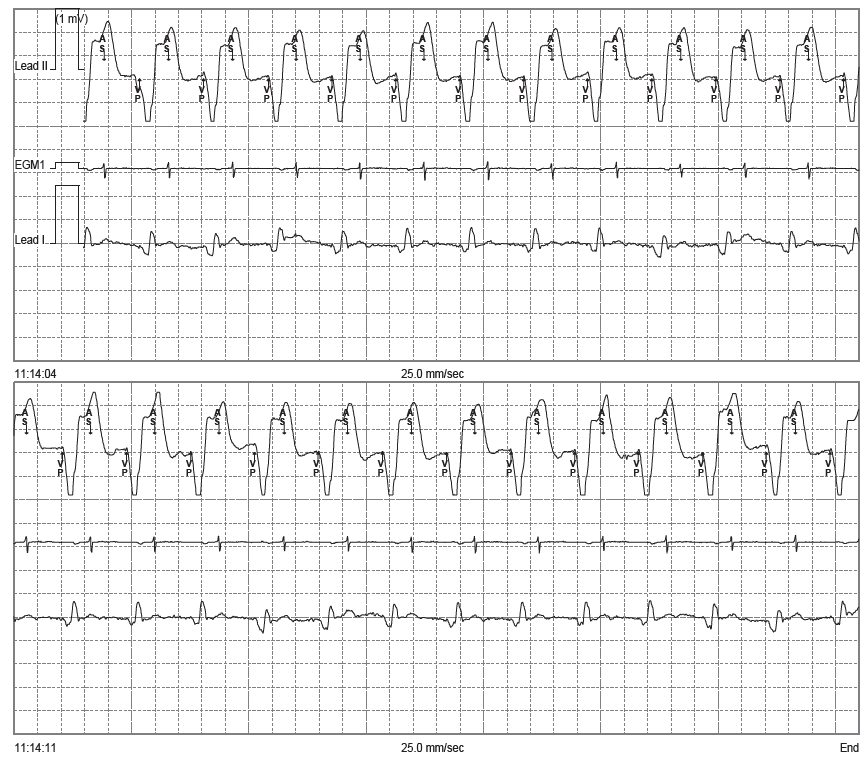
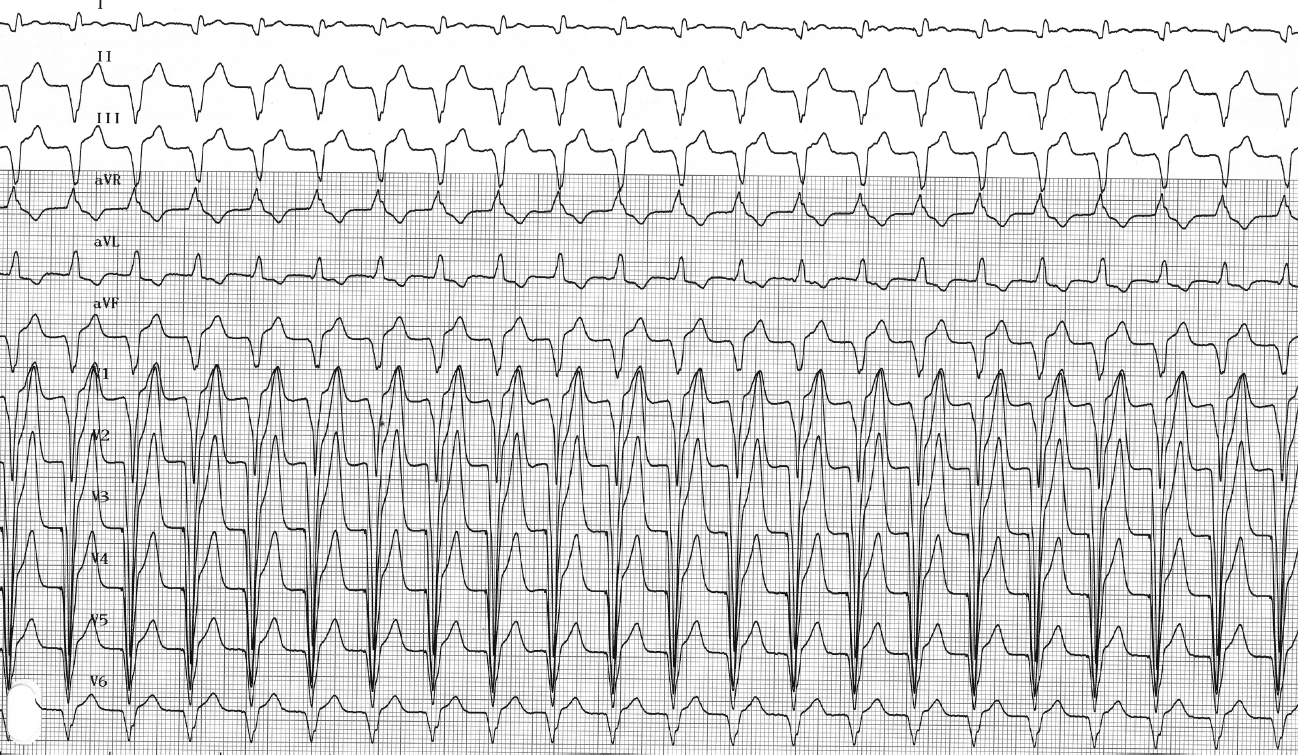
Trace description
Analysis of the EGM confirms the diagnosis of electrical reentry tachycardia: an uninterrupted sequence of VP-AS cycles (ventricular pacing, atrial sensing) with a prolonged AV delay to ensure that the maximum tracking rate is not exceeded;