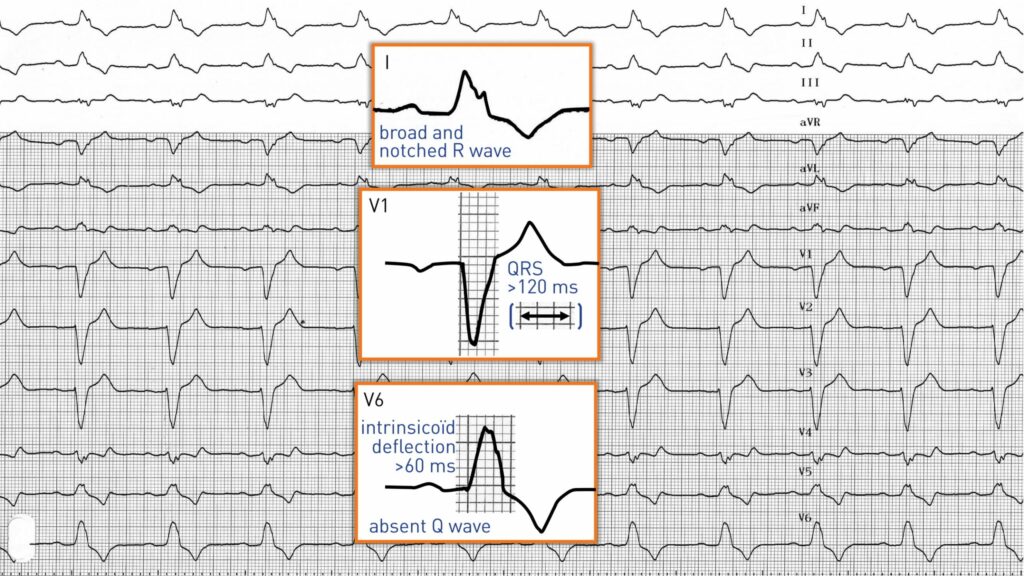
This patient presents a characteristic electrocardiographic pattern of left bundle branch block combining:
1. A widened QRS complex of 120 ms or more in adults, a QRS greater than 100 ms in children under 8 years of age;
2. A delayed onset of intrinsicoid deflection greater than 60 ms (ventricular activation time potentially reaching up to 100 ms) in the left precordial leads: this is due to the delayed depolarization of the affected ventricular wall; this is a major and fundamental criterion of left bundle branch block; the intrinsicoid deflection is normal in right precordial leads since the right ventricle is normally activated;
3. A characteristic QRS pattern in V6: an initial positive deflection is observed, with the direction of the septal depolarization being reversed and propagating from right to left; the septal activation vectors are thus directed to the left precordial leads which record a positive initial deflection; the presence of a q wave in V6 therefore allows to eliminate the diagnosis of a left bundle branch block; the amplitude of the R wave is often increased; indeed, when left ventricular activation is delayed, it no longer encounters opposition on the part of the right ventricular depolarization, accounting for a higher voltage potential; the foot of the R wave is often slurred or sometimes notched and the ensuing ascending branch is relatively fast and followed by a considerable strong slowing at the peak (bifidity or plateau pattern) and a brief descent towards the isoelectric line; absence of a terminal s wave;
4. A characteristic QRS pattern in V1: wide S wave in conjunction with the delayed occurrence of the left depolarization vectors; the most typical pattern is therefore rS or QS;
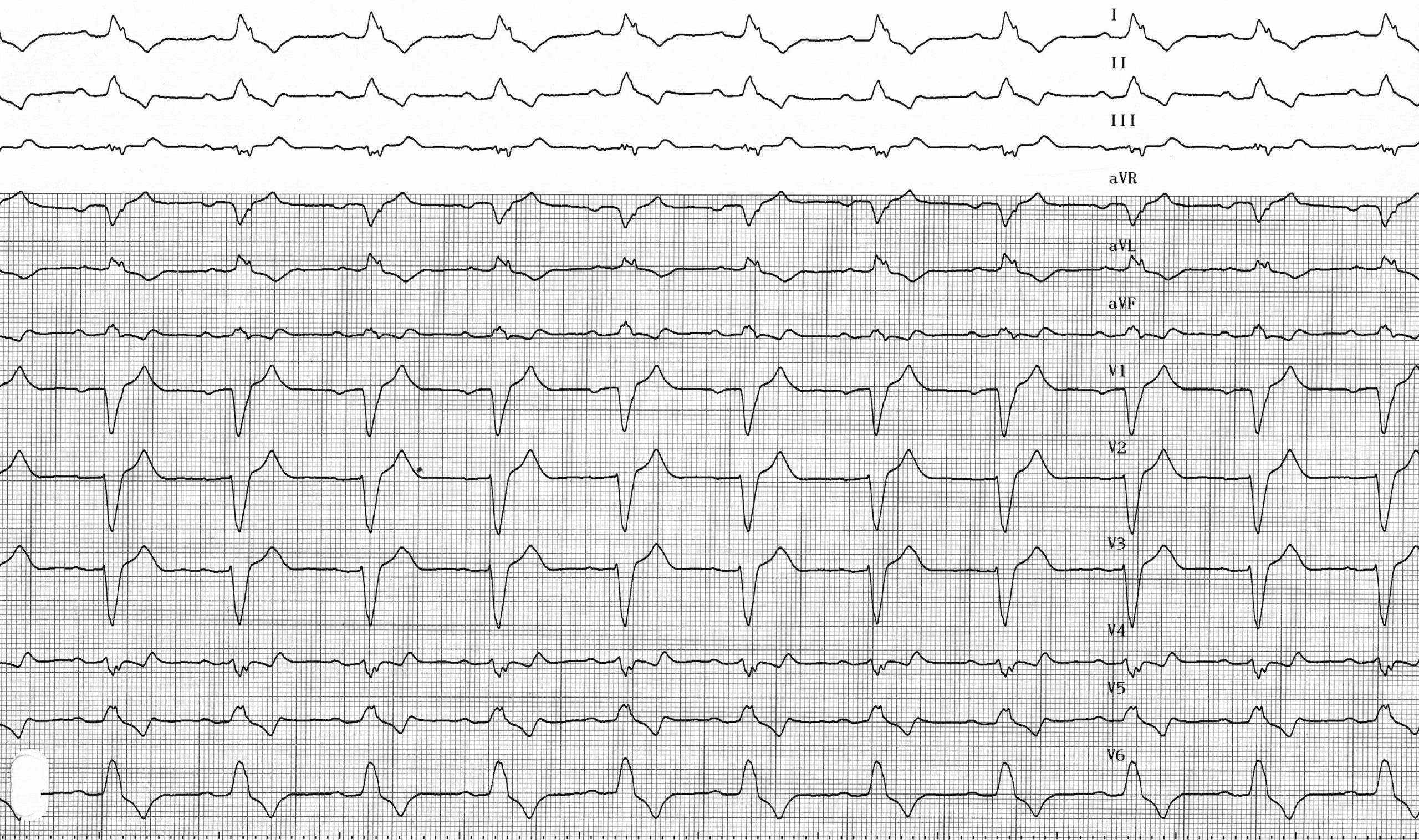
5. A modified ST segment and T wave in V5, V6: a depression of the ST segment and an inverted T wave are frequently found with a possible elevation in V1;
6. In the frontal leads, the characteristic pattern found in V6 (exclusive positivity followed by a negative and symmetrical T wave with depression) is found in lead I and more often in aVL;
QRS axis is variable: it can be normal or deviated to the left. The presence of a left bundle branch block renders the diagnosis of infarction or ventricular hypertrophy difficult.