A normal sinus rate corresponds by definition to a resting rate between 50-60 and 100 beats/minute. It is however common and of non-pathological nature to observe in daytime or more commonly at night, a slowing of the heart rate in an athletic or vagotonic person (sinus activity sometimes dropping under 40 beats/minute). It is common to define a sinus bradycardia (with or without escape rhythm) as pathological when it causes the onset of symptoms.
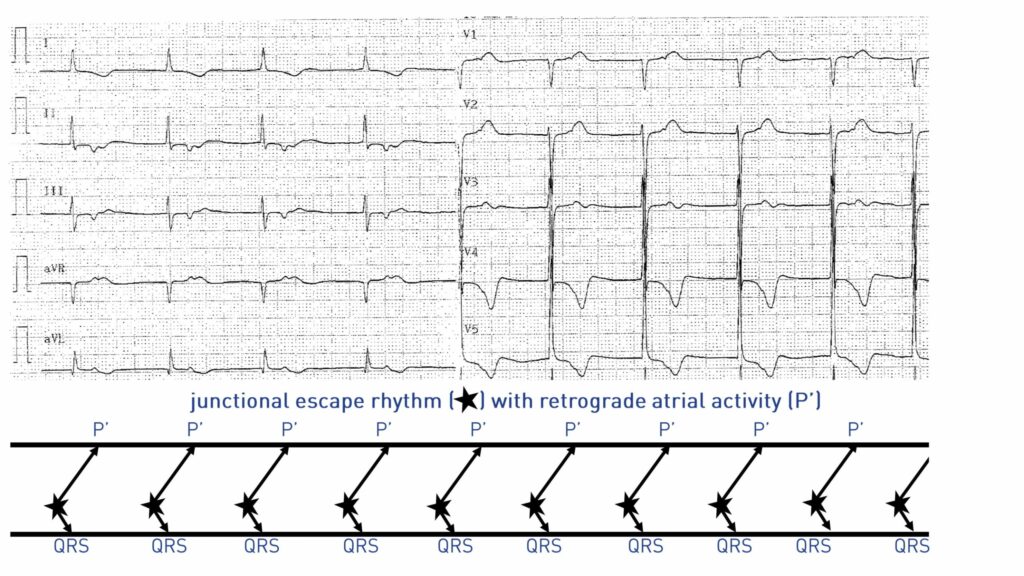
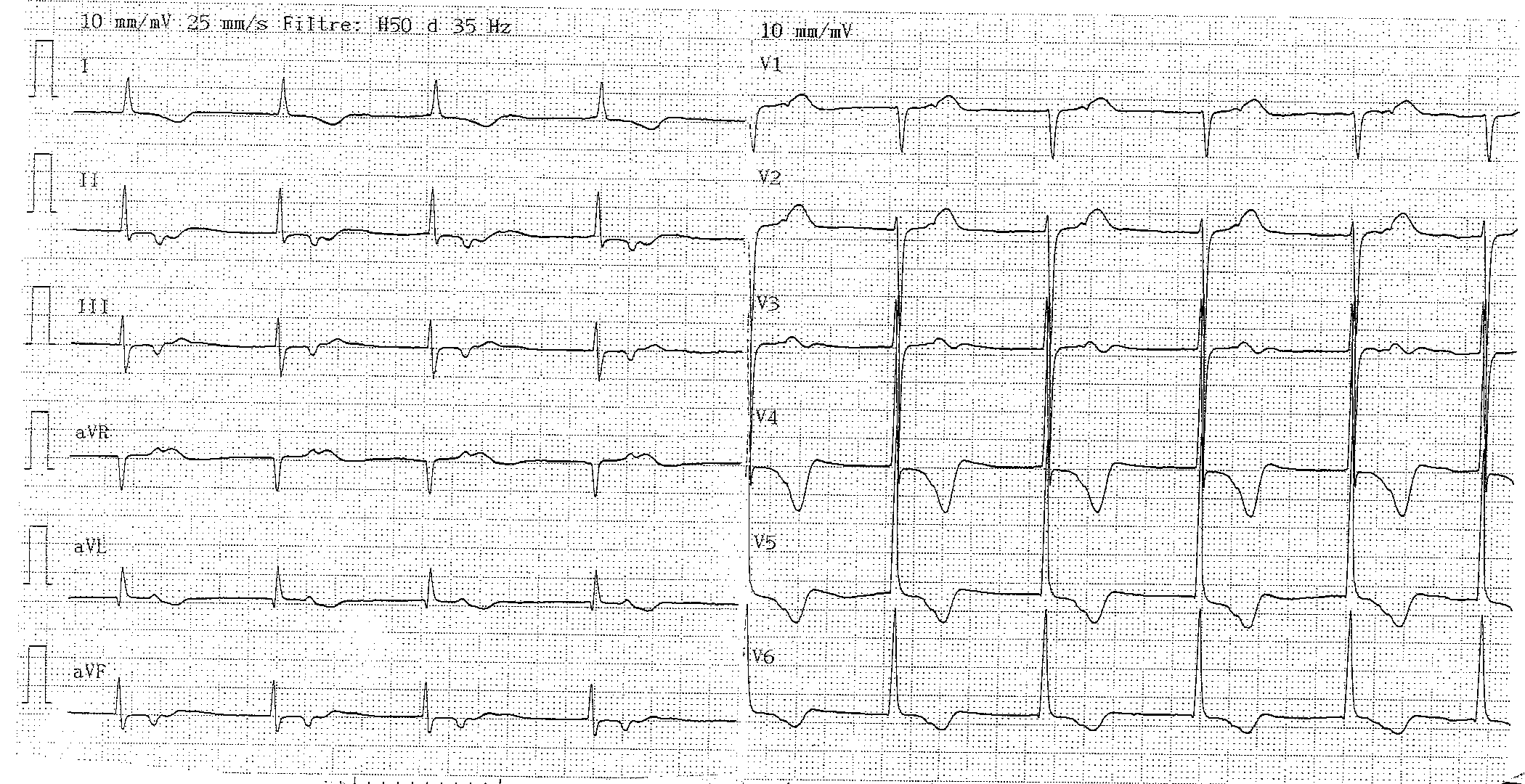
The tracing observed in this patient corresponds to a total absence of expression of sinus activity with junctional escape rhythm and retrograde atrial conduction. Two types of mechanisms may be involved: 1) absence of sinus impulses and 2) a sinus exit block at the atrial myocardium (3rd degree sinoatrial block). In the absence of sinus activity, ventricular depolarization can be initiated by a secondary automation center which generates the impulse by phase 4 spontaneous depolarization. In an episode of sinus node dysfunction, the ectopic focus is most often junctional and is located in the inferior portion of the atrioventricular node or the adjacent portion of the common trunk of the bundle of His called the nodo-Hisian region. If no junctional focus appears, a ventricular focus (inferiorly located, wide QRS) or occasionally another slow atrial focus (most often a coronary sinus focus, with negative atrial activity in the inferior leads) may act as a back-up pacemaker. When the escape is junctional, the appearance of the QRS complex is usually unchanged from that observed when the rhythm is sinus. In rare cases, a slightly modified pattern can be observed, although the mechanisms for these discrete morphological differences are not fully established.