Trace 2.6: Differential diganosis of sinus dysfunction
Patient information
67-year-old man with a history of atrial fibrillation referred to the department due to discovery of irregular bradycardia suggesting the need for implanting a pacemaker;
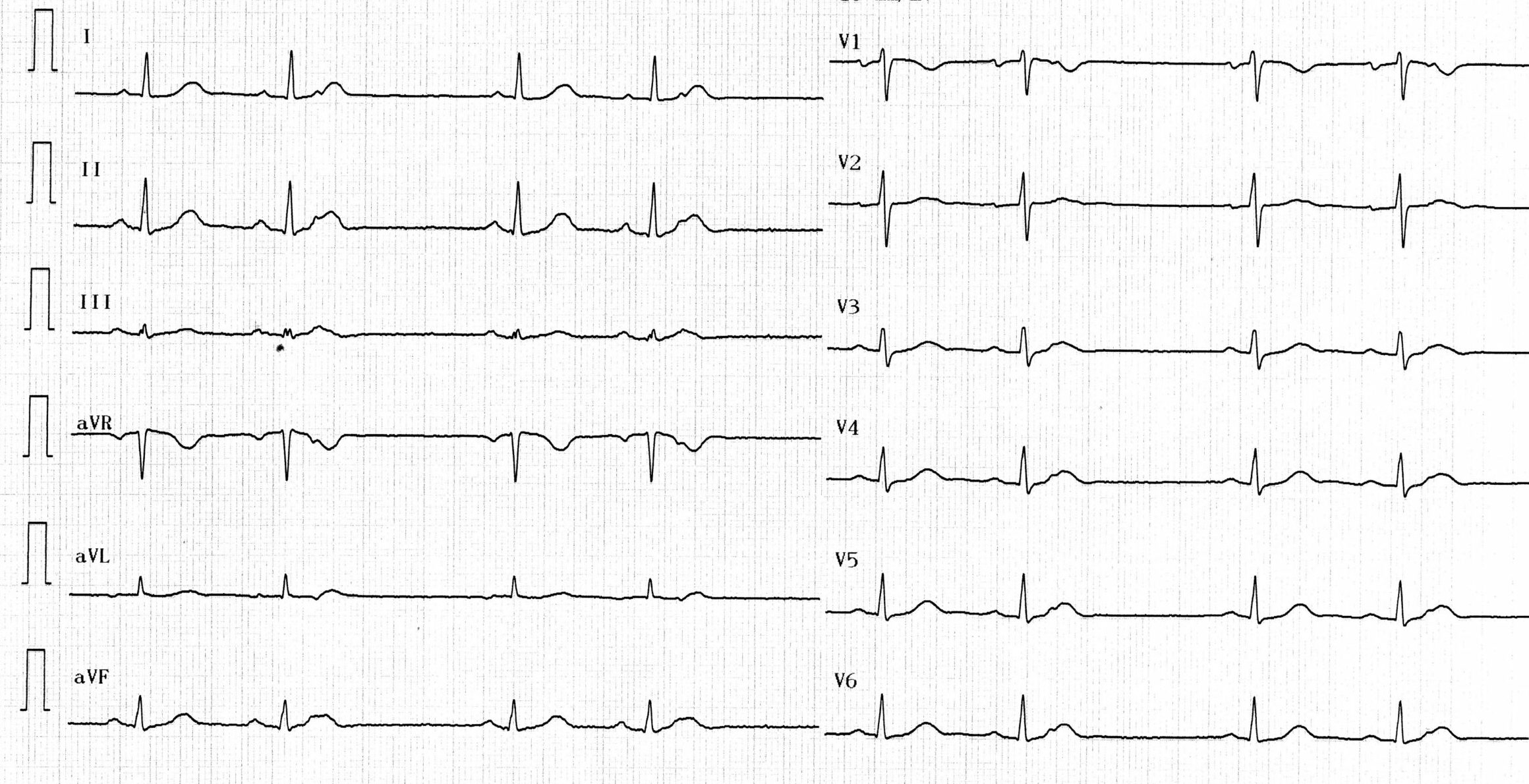
ECG
Question
Regarding this ECG, which answer(s) is(are) true?
Commentaires
ECG description
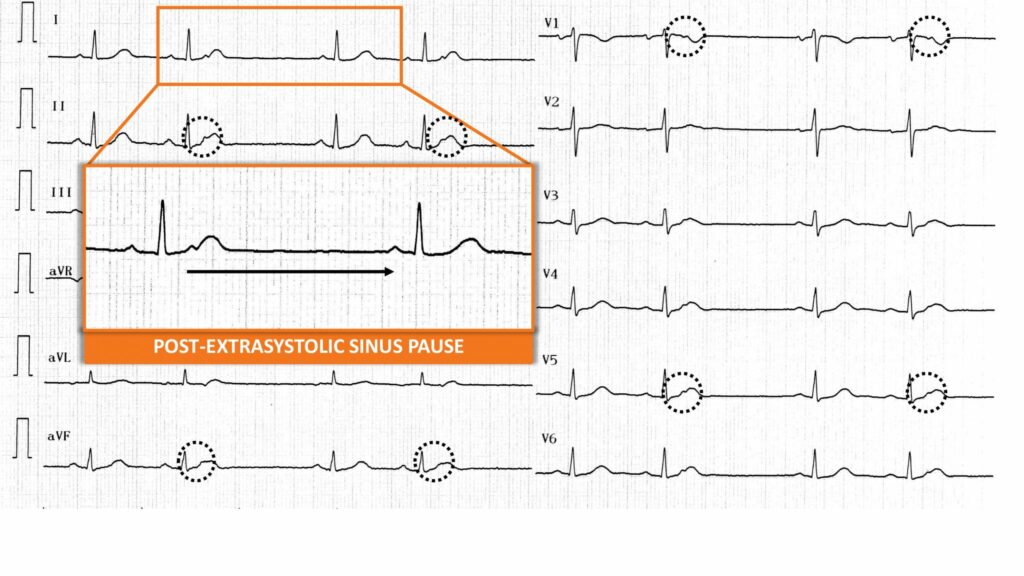
Sinus activity (positive in leads I, II, V5, V6 and negative in aVR) with significant RR interval variability; in the initial portion of the T wave, there is an ectopic atrial activity corresponding to a blocked atrial extrasystole (not followed by a QRS) with a post-extrasystolic sinus pause explaining the pseudo sinus bradycardia;
Explication
This patient was referred due to irregular heart rate and “sinus pauses”. A careful inspection of the tracing allows the highlighting of a notch in the T wave preceding the pause corresponding to a blocked atrial extrasystole explaining the ensuing post-extrasystolic pause. It is therefore not an issue of depressed automaticity (sinus node dysfunction and discussion on the need for a pacemaker implantation) but rather of a hyper-automaticty (atrial extrasystole and discussion on the relevance of an antiarrhythmic therapy). A blocked atrial extrasystole thus constitutes the differential diagnosis of sinus node dysfunction and should be systematically investigated when in the presence of a pause, the therapeutic consequences being drastically opposite.
To remember
An atrial premature complex 1) can be difficult to identify on the electrocardiogram because it may be “concealed” within the T wave and non-conducted, 2) evokes the differential diagnosis of sinus pause, 3) may originate from a focus located at the ostium of one of the pulmonary veins and represent the trigger for the induction of atrial arrhythmia episodes.