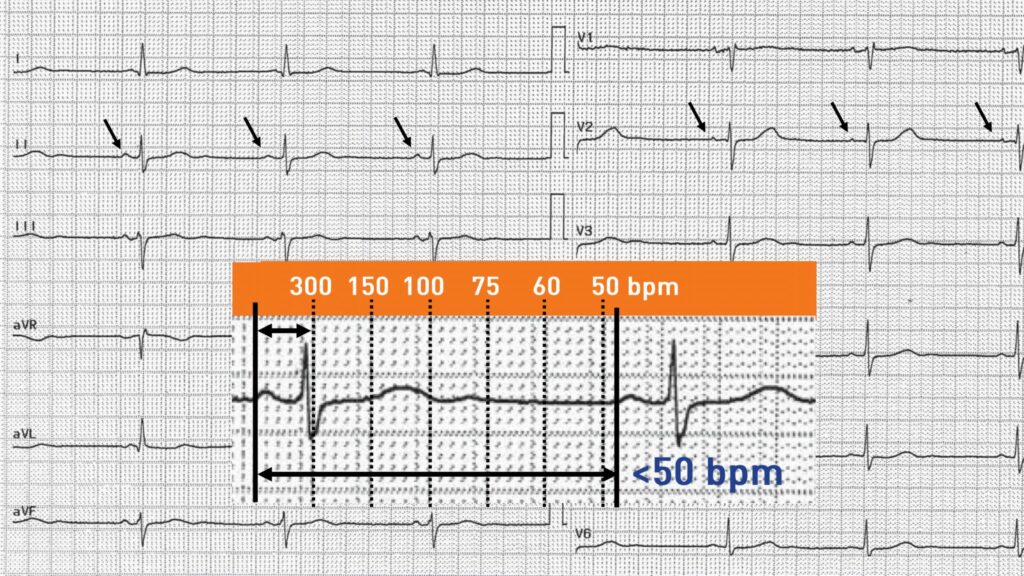
This patient has a sinus bradycardia corresponding to a heart rate lower than 50 or 60 bpm (depending on definitions) at rest. The difference between physiological and pathological bradycardia may be difficult to determine. Indeed, a vagal hypertonia frequently observed in athletic patients can explain a physiological bradycardia without the need for special investigations or treatment. A drug etiology is also frequently observed (beta-blocker, digoxin, amiodarone, calcium channel blocker, etc). The pathological nature and therapeutic response (pacemaker implantation) are therefore determined by the presence of symptoms that can vary in severity and specificity (syncope, lipothymia, asthenia, vertigo). A chronotropic incompetence (defined as the inability to reach a heart rate at exercise exceeding 70, 80 or 85% of the theoretical maximum rate depending on definitions) may be accompanied by symptoms appearing only on exercise (limitation of exercise capacity, exertional dyspnea).
It was decided not to implant this asymptomatic patient presenting a preserved chronotropic function (normal acceleration of the heart rate to exercise) but to monitor him with regular Holter-ECG recordings to screen for more marked paroxysmal bradycardias. Beta-blocker or calcium bradycardia inhibitor treatment should not be recommended for his hypertension.