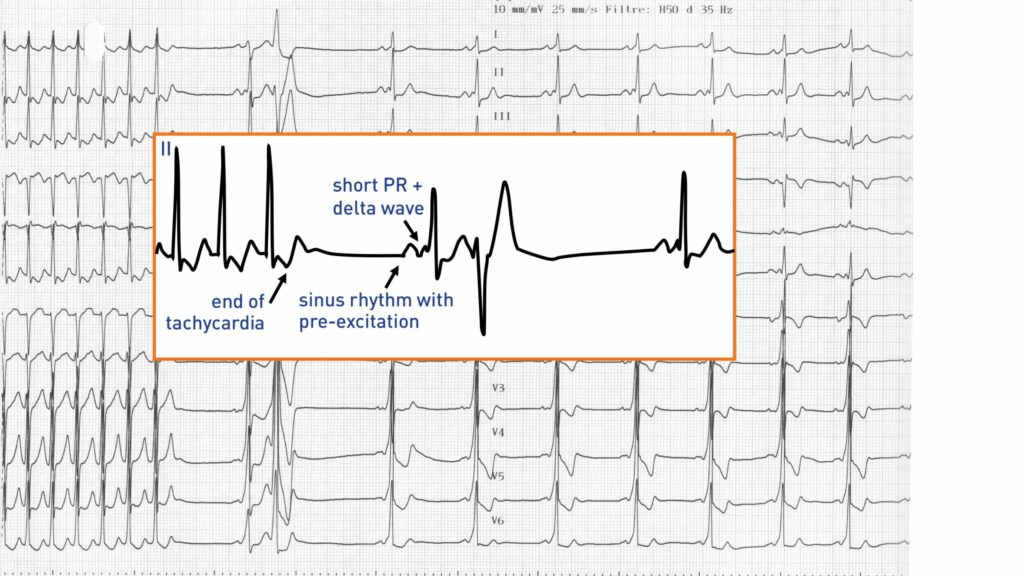
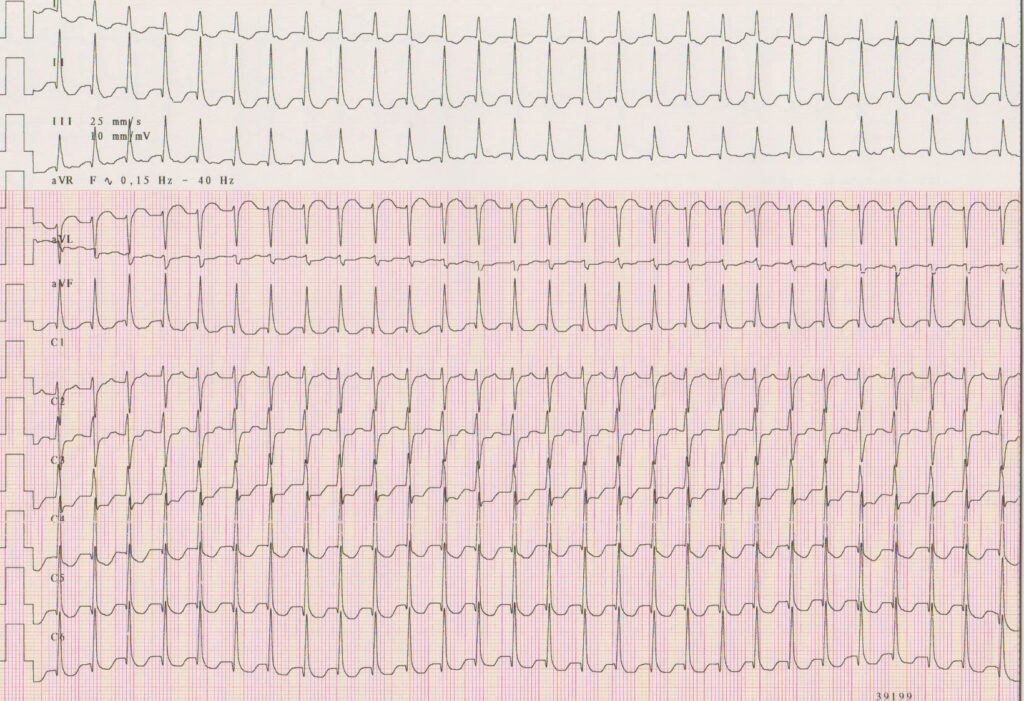
Trace description
The termination of the tachycardia was not recorded; after the return to sinus rhythm, short PR pattern without obvious pre-excitation, possible sequela of inferior and anterolateral necrosis;
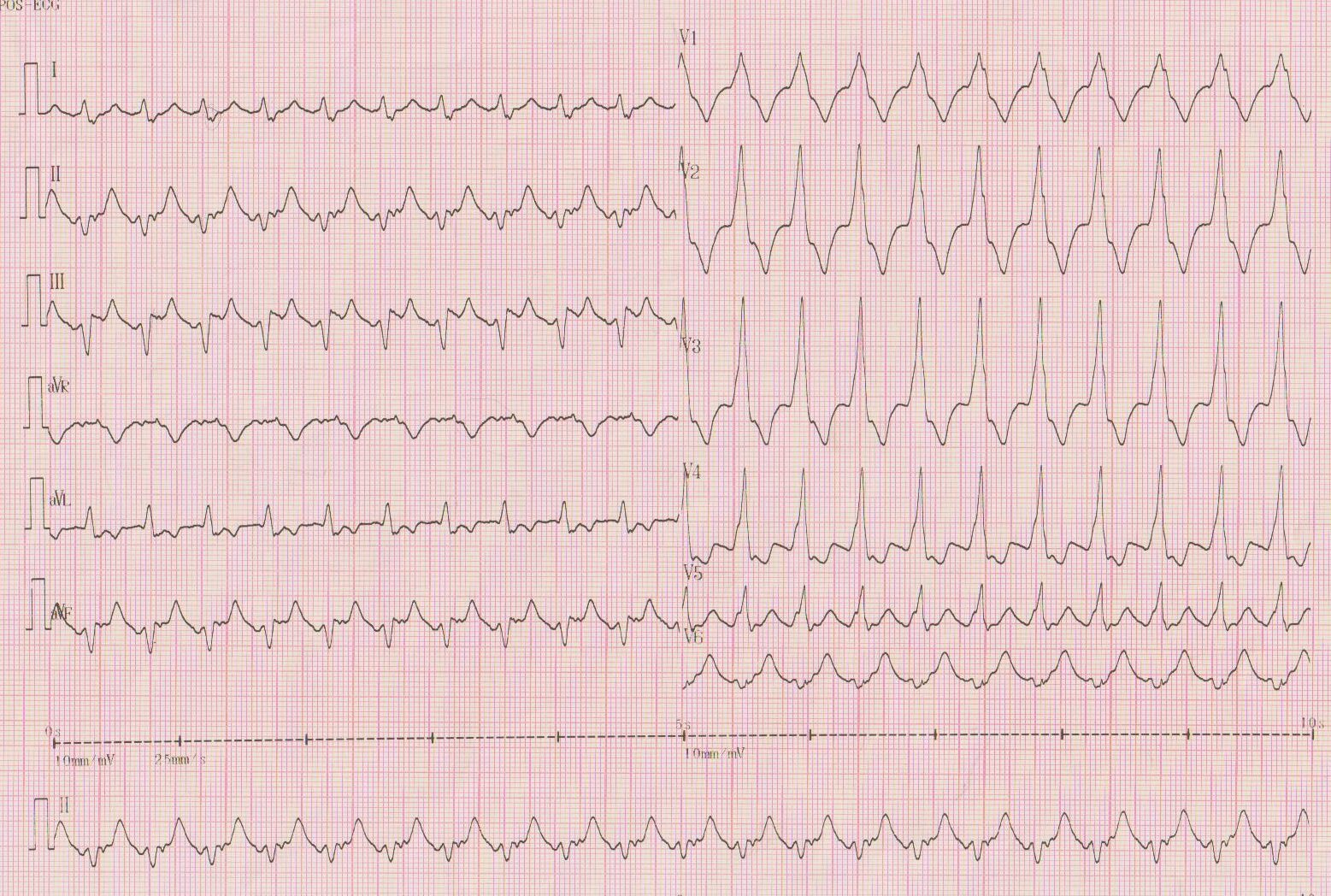
Trace description
During the hospitalization, a new episode of tachycardia; narrow QRS tachycardia;
Commentary
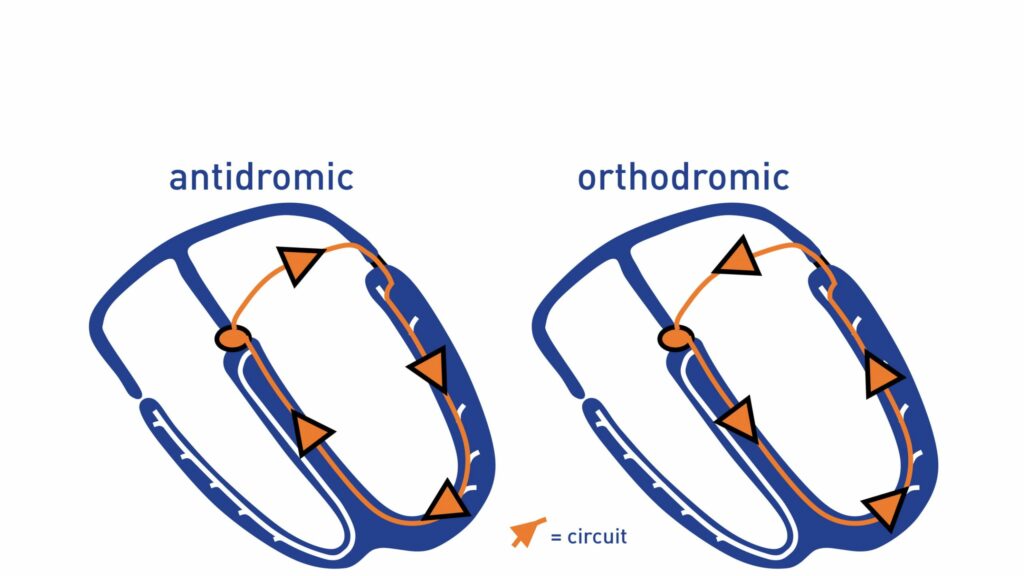
This patient presented a masked left lateral accessory pathway (anterograde conduction only visible after Adenosine injection) and episodes of orthodromic (narrow QRS) and antidromic (broad QRS, major pre-excitation pattern) tachycardia. This clinical case illustrates the difficulty of diagnosing an antidromic tachycardia mistaken for a ventricular tachycardia.
Orthodromic tachycardias are the most common arrhythmias encountered clinically in patients with Wolff-Parkinson-White syndrome. Antidromic tachycardias, in which the circuit is reversed, are much rarer since only documented in approximately 5% of patients with accessory pathway or in less than 10% of patients with inducible tachycardias in the electrophysiology laboratory. The impulse descends from the atrium to the ventricles through an accessory bundle (anterograde conduction) and ascends toward the atrium in a retrograde manner through the nodo-Hisian pathway before once again descending through the accessory pathway. In rare cases, the impulse may ascend back to the atria through a second accessory pathway. The onset of this type of tachycardia requires a unidirectional block in one of the two atrioventricular conduction pathways. Unlike orthodromic tachycardias, an atrial extrasystole is conducted in anterograde manner through the bundle of Kent but is blocked by the normal pathways, or a ventricular extrasystole ascends through normal conduction pathways but is blocked in the bundle of Kent. Various studies suggest that antidromic tachycardias are preferentially observed in patients with multiple accessory pathways or with a lateral accessory pathway located remotely from the atrioventricular node. It appears that in order to induce this arrhythmia, a minimum critical distance is necessary, the impulse needing to be blocked in the node, conducted through the accessory pathway, reach the ventricular apex and then return back up to the node to allow retrograde conduction to the atria without encountering the conduction pathways in refractory period.
The management of antidromic tachycardias is sometimes difficult given their rarity and their electrocardiographic pattern of wide QRS tachycardia (ventricular activation is exclusively through the accessory pathway), which can lead to suspecting the diagnosis of ventricular tachycardia.
An antidromic tachycardia presents a poorly-specific electrocardiographic pattern that must be differentiated from a 1:1 supraventricular arrhythmia with conduction aberration and a ventricular tachycardia with retrograde conduction. The diagnosis is sometimes difficult, as in this patient, when the presence of the accessory pathway is unknown and that the pre-excitation is not visible on the sinus complexes (masked left lateral pathway).
The electrocardiogram shows:
The highlighting of antidromic tachycardia may constitute a factor of poor prognosis since it is associated with an increased risk of malignant forms. Indeed, this type of tachycardia is more frequently observed in patients with multiple accessory pathways. In addition, it appears that the occurrence of antidromic tachycardia is a marker of good conductivity throughout the pathway.
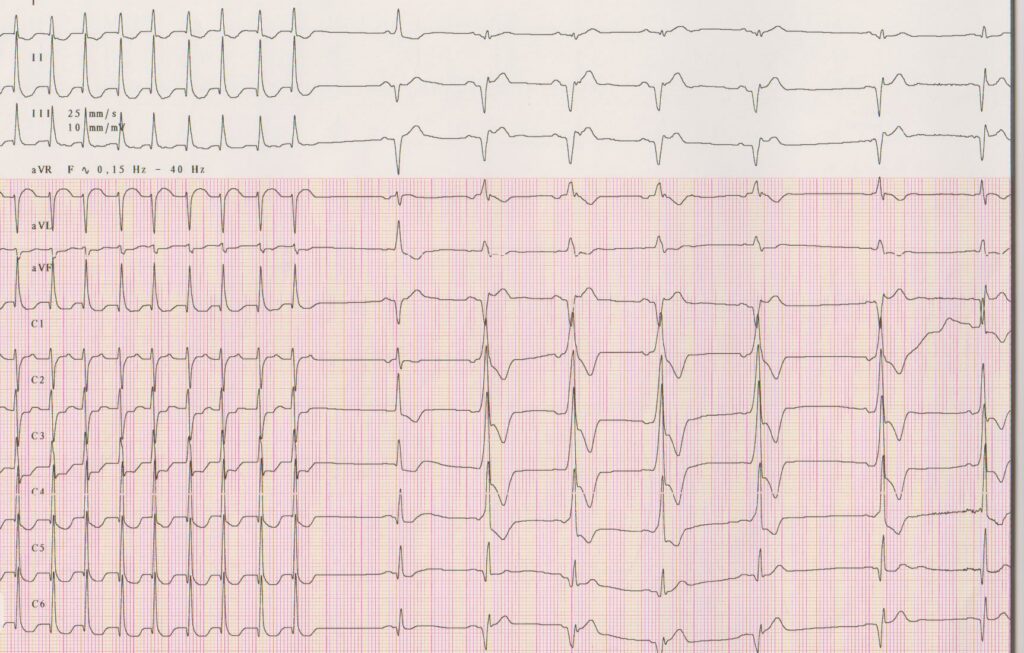
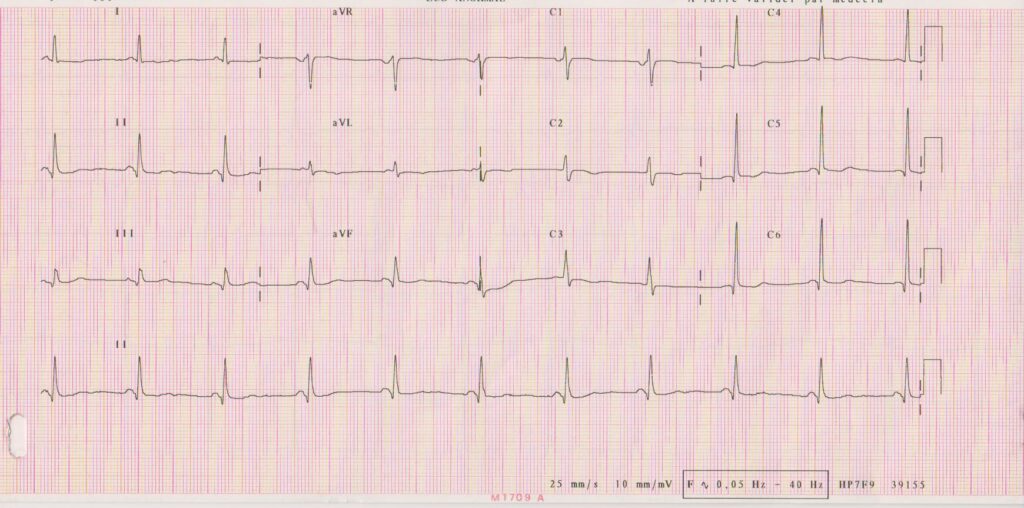
Trace description
Interruption of the tachycardia upon injection of 6 mg Adenosine; after return to sinus rhythm, evidence of major pre-excitation which was masked on the previous sinus rhythm tracing; the conduction through the atrioventricular node was completely blocked by the injection of Adenosine, the conduction is now exclusively through the accessory pathway; the QRS pattern is identical to that observed on the first tachycardia suggesting that it was an antidromic tachycardia;