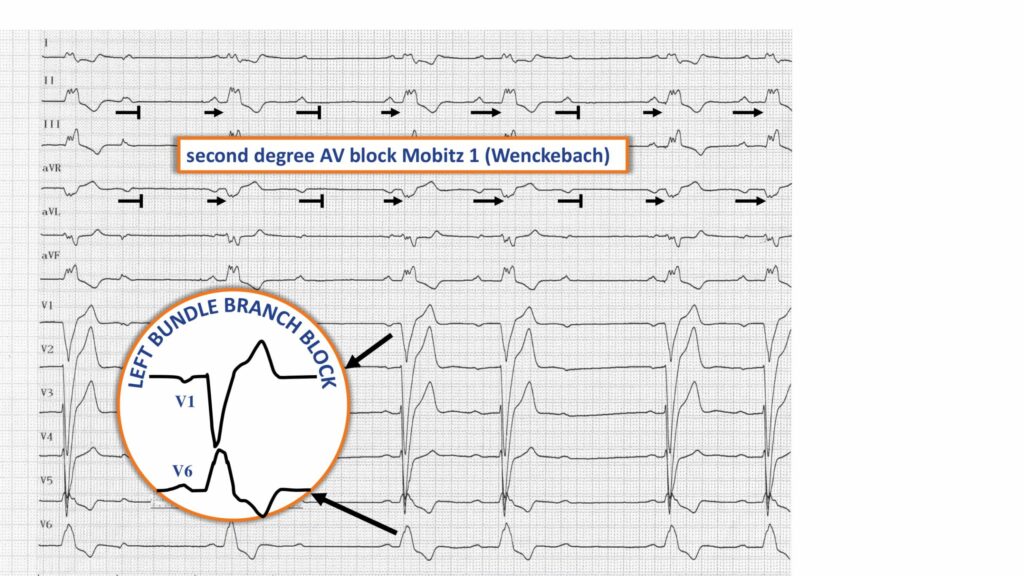
During an episode of near-syncope
Trace
Left bundle branch block; bradycardia associated with a Mobitz 1 second-degree AV block pattern; gradual prolongation of the PR interval followed by blocked P wave (Wenckebach periods);
Commentary
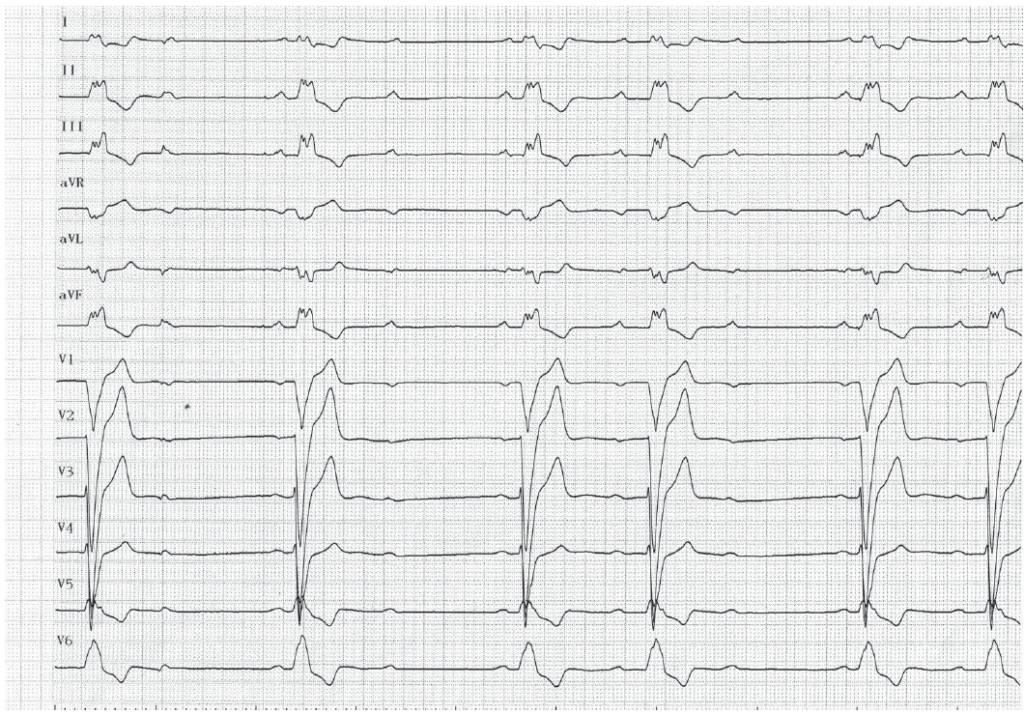
This patient presented with a syncope which resulted in a fall with bleeding scalp wound. The electrocardiogram revealed a characteristic pattern of complete left bundle branch block. During an episode of lightheadedness, the ECG showed a bradycardia in conjunction with a second-degree (Mobitz 1) AV block pattern.
When there is an associated branch block, a second-degree AV block with Wenckebach periodicity may result from a slowing of conduction in the atrioventricular node, but should also raise suspicion and warrant investigation for a delayed activation on the branch opposite to the blocked branch (trifascicular block). The infra-Hisian Wenckebach periods in these instances are associated with a constant AH interval and a gradual prolongation of the HV interval, the blocked P wave being followed by a His potential not conducted to the ventricle.
The indications for implantation in the setting of second-degree AV block type 1 are controversial. The causal relationship between conduction disorder and the onset of symptoms is difficult to establish, especially when the symptoms are modest and unspecific. There is a class IIA indication in the European guidelines when a second-degree AV block type 1 is responsible for symptoms or when the conduction disorder is of intra- or infra-Hisian localization (major risk of progression to a complete atrioventricular block) upon electrophysiological study (EPS). This patient underwent an EPS which confirmed the presence of a trifascicular block and underwent pacemaker implantation.