Trace description
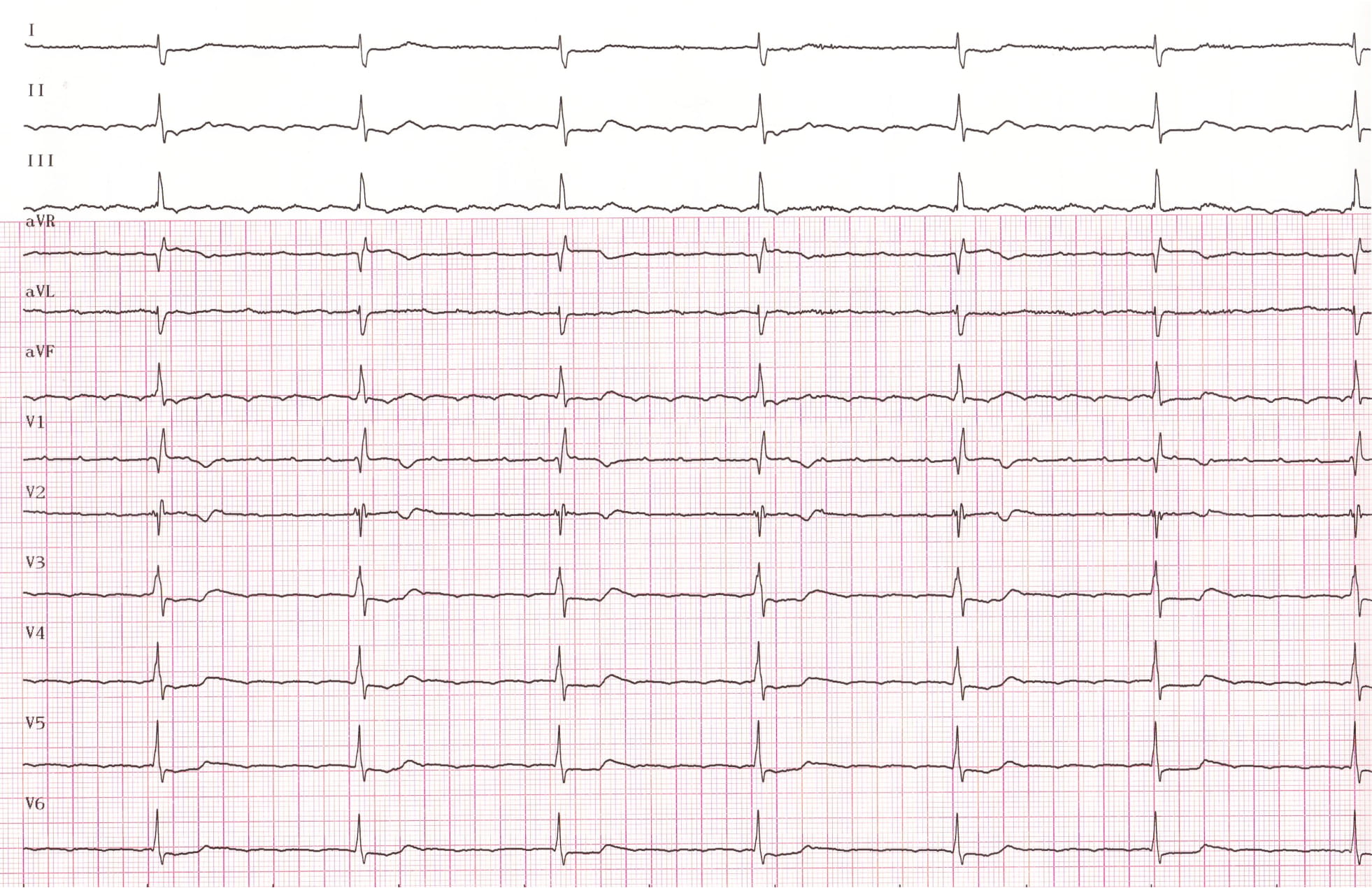
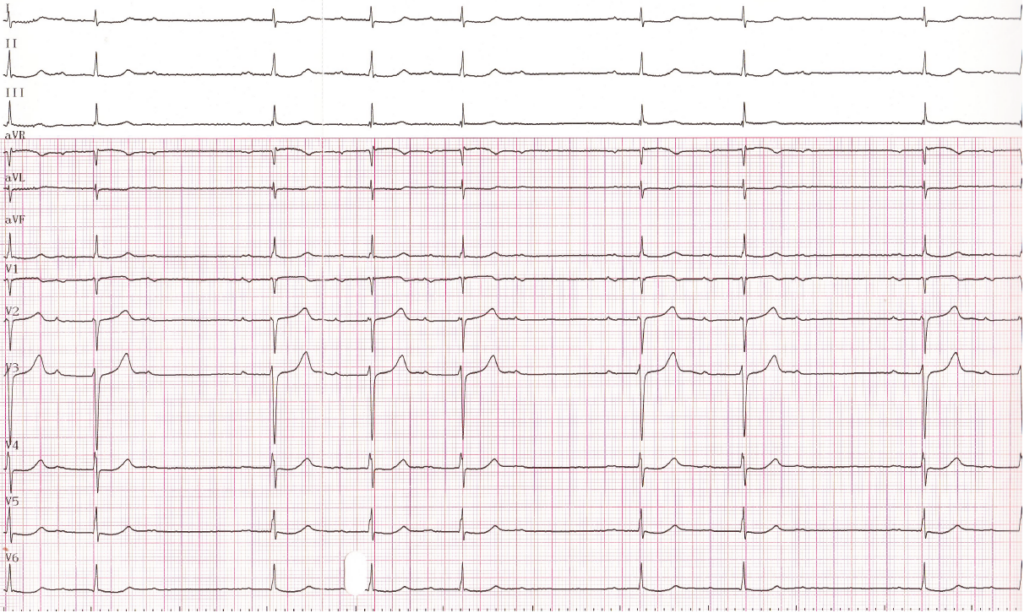
This patient underwent an ablation of the cavo-tricuspid isthmus; the next tracing was recorded after the ablation procedure.
Question
What do we see on the second ECG?
A. left bundle branch block
B. right bundle branch block + left anterior hemiblock
C. thirddegree AV-block
D. second degree AV block type Mobitz 2
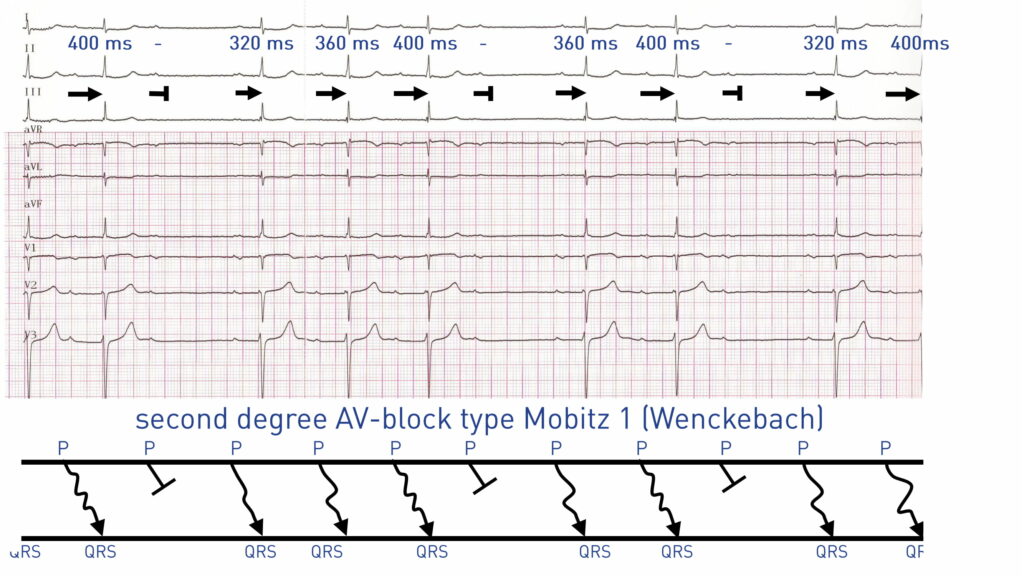
E. second degree AV block type Mobitz 1
Correct answer: E. Atrial sinus activity and second-degree AV block with Wenckebach periodicity;
Commentaires
This patient presented an atrial flutter and a high-grade atrioventricular conduction disorder, which is characterized by a slow ventricular rate and a lack of direct relationship between atrial activities and ventricular activities. The highlighting of a second-degree AV block after return to sinus rhythm confirms the presence of this likely junctional conduction disorder (Wenckebach periods with a significant increment in PR interval suggesting a nodal block). This patient was not under any treatment aimed at slowing atrioventricular conduction. The electrical pattern evolved toward an escalation of the conduction disorder with 2:1 atrioventricular rhythm and symptomatic bradycardia of 30 beats/minute. The patient therefore underwent implantation of a dual-chamber pacemaker.