

Boston Scientific subcutaneous ICD - Counters and Detection
Content
The methods used to detect and classify cardiac cycles differ completely between an intracardiac defibrillator and a subcutaneous defibrillator. Indeed, while the main purpose of a subcutaneous defibrillator is to correctly detect, without significant delay, an episode of ventricular arrhythmia that could compromise the patient’s survival, there is no absolute need to correctly classify each cycle as sinus rhythm or arrhythmia. Analysis of the tracings frequently reveals oversensed cycles, undersensed or incorrectly classified rapid cycles (e.g., ventricular extrasystoles classified as sinus rhythm), which could be problematic for an intracardiac defibrillator that provides pacemaker function requiring perfect detection of all cycles to avoid stimulation during vulnerable periods. The two priorities for a subcutaneous defibrillator are therefore to avoid inappropriate therapies due to oversensing of the T wave in sinus rhythm while maintaining the ability to detect rapid rhythms, which justifies the use of different sensitivity profiles depending on the heart rate. There are also a number of fundamental differences in the amplitude and shape of the signals detected by a subcutaneous defibrillator compared to the signals detected by an intracardiac defibrillator. These different elements explain certain differences in operation and programming:
- The slope and frequency of signals recorded by subcutaneous electrodes are lower in sinus rhythm, leading to the recording of “softer” QRS complexes that are less differentiated from the T wave or P wave. The high-pass filter value is lower in a subcutaneous defibrillator than in an intracardiac defibrillator (3 Hz vs. 14–20 Hz).
- The signals recorded by subcutaneous electrodes are broader than intracavitary signals, justifying the use of a longer post-detection refractory period to avoid double counting of the R wave. The duration of the refractory period varies according to the frequency of the detected cycles (shorter in the shock zone) so as not to limit the ability to detect very fast rhythms while minimizing the risk of oversensing in sinus rhythm. The refractory period value is not programmable (160 ms for the shock zone, 200 ms for cycles slower than the shock zone). – A subcutaneous defibrillator operates with a higher maximum sensitivity value than an intracardiac defibrillator (0.08 mV versus 0.3 to 0.6 mV). as the amplitude of intracardiac signals recorded by subcutaneous electrodes is generally lower (QRS complex amplitude of 0.3 to 3.6 mV in sinus rhythm); the maximum sensitivity level is not programmable (0.08 mV, 80 µV) and remains the same regardless of the frequency of the signals detected and certified.
- The signal-to-noise ratio, which corresponds to the difference between the amplitude of the signal to be detected (QRS complex) and the amplitude of the “noise” (P wave, T wave, myopotentials, electromagnetic interference), is lower; this is because, as explained above, the amplitude of the QRS complexes is lower. in addition, extracardiac signals have a higher amplitude, as the subcutaneous electrodes are much further apart than the bipolar electrodes of an endocavitary probe; proper functioning therefore requires the use of specific filters to reject high-frequency signals such as 50 or 60 Hz; Once the signal is detected, the certification phase classifies the cycle as certified or as noise/oversensing. Signals with too high a frequency (myopotentials, interference, probe fracture) are classified as noise and are excluded from the heart rate calculation. The signals then go through four additional certification steps to diagnose double counting of the R wave or oversensing of the T wave.
- Postural variations in the amplitude and appearance of QRS complexes are more pronounced than with an endocardial defibrillator, requiring the use of a corrective algorithm to mitigate these variations.
- Dynamic sensitivity is used to reduce the risk of T wave oversensing; once the signals have been filtered, the device uses an adaptive detection threshold based on the amplitude of the two previous certified cycles; the sensitivity level increases in parallel with the increase in heart rate to optimize detection capabilities during tachycardia. Different sensitivity profiles (refractory period, adaptation level, adaptation delay) are used depending on the frequency of the detected signals, the programming (single zone or two zones), and the similarity of the amplitude of the two previous certified signals. None of these parameters are programmable. When the rhythm is slow, the priority is to minimize the risk of T wave oversensing, so the sensitivity profile is adjusted (long refractory periods, high adaptation level, adaptation delay extended especially when the amplitude of the two previous certified complexes is different). In the shock zone, the main objective is to optimize the detection of possible ventricular fibrillation with rapid signals of variable amplitude, which requires the use of a shorter refractory period, a relatively low adaptation level, and a short adaptation delay.
- A subcutaneous defibrillator does not provide long-term pacemaker function, which considerably limits the constraints in terms of the need for correct cycle-to-cycle detection of all signals (no risk of stimulation during the vulnerable period). This allows the use of a system that averages over several cycles. During the decision phase, the device examines all certified cycles and continuously calculates a ventricular rate average over four certified RR cycles. For a cycle to be considered fast, the average of the four cycles must be fast.
- In addition to a shock zone, the device allows for a conditional shock zone using two morphology analysis algorithms and one QRS duration measurement algorithm to distinguish between ventricular arrhythmias and supraventricular arrhythmias. The existence of relatively distant detection electrodes allows for reliable analysis of signal morphology, albeit with greater postural variability. As explained above, programming a conditional shock zone not only introduces a discrimination zone but also modifies the detection profile.
Counter
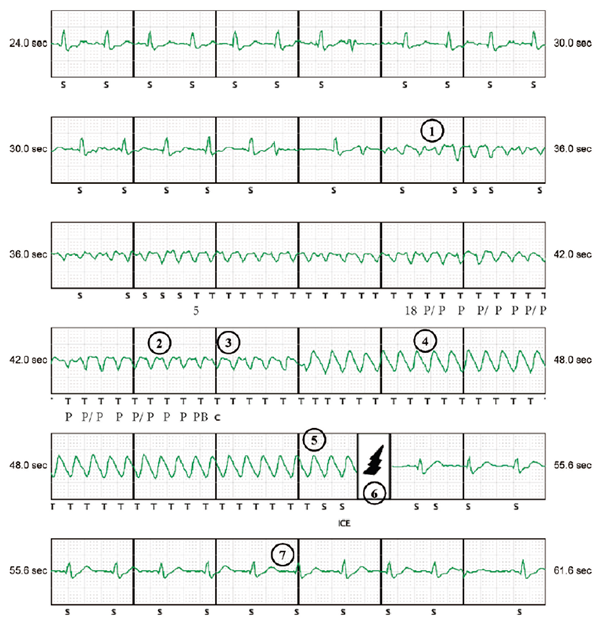
The initial probabilistic counter is non-programmable, non-modifiable, and requires 75% of fast cycles classified as T. In fact, a rolling window of the 24 most recent intervals defined by certified events are constantly analyzed. The initial counter is checked if 18 of the 24 most recent intervals are classified as T. Before starting the charge, the persistence criterion must then be checked and the last 2 raw intervals must correspond to one of the tachycardia zones. Before the capacitors begin charging, it is therefore necessary that:
- the X/Y probabilistic counter be filled; a rolling window of the last 24 certified cycles be analyzed; it should be noted that the first cycle of tachycardia classified as T indicates a counter at 5 (to compensate for the fact that the classification is based on the average of 4 cycles); ventricular fibrillation is by definition a rapid, anarchic, chaotic arrhythmia with low-amplitude and/or variable-amplitude ventricular signals; The specific characteristics of detection in this type of device (long refractory periods, adaptive sensitivity profile that varies according to the frequency and amplitude variability of consecutive cycles) increase the risk of under-detection. This ratio of 75% between fast and slow cycles was chosen in order to achieve an optimal balance between correct detection of ventricular fibrillation
- A minimum of 16 cycles classified as T are also required.
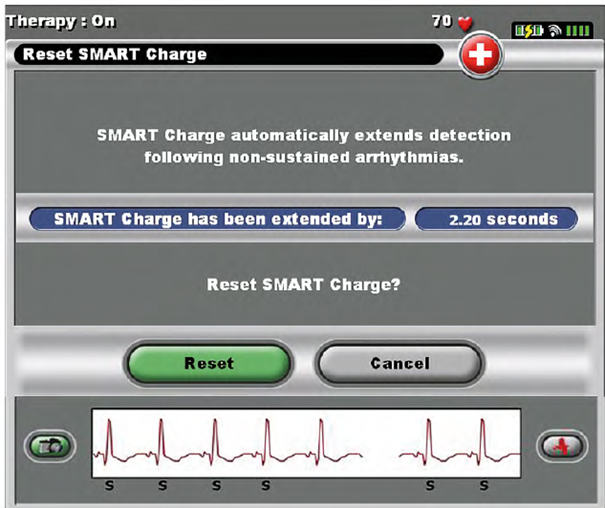
- The persistence criterion must be verified. Once the X/Y criterion has been validated, a minimum persistence of 2 cycles with a ratio of 18/24 must be verified in order to avoid unnecessary charging. The last cycle of the 18/24 counter counts as the first cycle of persistence. The Smart Charge algorithm ensures that each diverted charge (untreated episode) increases this persistence by 3 cycles with a maximum of 5 increases, which allows the device to delay the charging of the capacitors if the arrhythmia is not sustained. During persistence, the 18/24 T cycle criterion must be verified on all cycles. the duration of persistence can therefore be a maximum of 17 cycles; the total extension (in seconds) is indicated on the programmer during interrogation; the extension value can be reset to 0 using the programmer; the Smart Charge algorithm cannot be disabled; this extension of persistence only applies to the first shock of an episode (not for pulses 2 to 5).
The last two cycles (gross intervals) before the start of charging must be fast;
- after persistence, an additional beat is still required before starting charging (Processing Beat). Once the shock has been delivered, two counters compete:
- the end-of-episode counter, which requires 24 consecutive certified cycles classified as S (cycles marked “•” or “N” do not interfere with this counter).
Detection delay
Subcutaneous defibrillators were developed to enable the correct detection of a VF episode as a whole rather than precise cycle-by-cycle detection, as the correct classification of each ventricular cycle is less critical than for an intracardiac defibrillator. This leads to a longer detection delay than with a traditional defibrillator, with more marked interindividual variability. Literature reports an average time between the onset of arrhythmia and the delivery of the shock of approximately 14 seconds for a subcutaneous defibrillator, which is longer than for an intracavitary defibrillator, with greater variability between patients. This delay is broken down into the initial time taken to detect the arrhythmia, the time taken to charge the capacitors, and the time taken to confirm the arrhythmia at the end of charging. The charging time for 80 joules is generally less than 10 seconds at the beginning of the device’s life and remains less than 15 seconds when the case is changed. An electric shock is delivered by a subcutaneous defibrillator after less than 18 seconds in 88% of cases and less than 21 seconds in 95% of cases.
The latest recommendations, based on all recent studies, suggest the need to avoid treating organized and slower ventricular arrhythmias too early and too aggressively. Programming the number of cycles required for initial detection in an intracardiac defibrillator is crucial for the patient’s quality of life, prognosis, and also for the device’s lifespan. The issue for subcutaneous defibrillators is significantly different. The only therapy option available is electric shock without the possibility of anti-tachycardia pacing. In addition, the initial probabilistic counter (18/24) cannot be changed. When a detection delay is observed, this is not a programming choice but the result of repeated detection failures most often observed at the beginning of an episode. As explained above, the sensitivity profile changes according to heart rate, which may explain the detection delay most often observed at the beginning of an episode:
- Fast profile: in the shock zone, the objective is to optimize the detection of possible ventricular fibrillation with fast signals of variable amplitude. The post-detection refractory period is 160 ms, then the sensitivity level starts at 60% of the average amplitude of the two preceding cycles (fixed level for 80 ms) and then increases (decrease in sensitivity value to 37.5% of the average amplitude of the two preceding cycles for 4 ms). Sensitivity then increases with a decrease in this value according to an exponential curve up to a value of 0.08 mV.
- Average profile: this profile, with a longer blanking period than in the shock zone (200 ms) and a high sensitivity level, is applied for tachycardias that are slower than those in the shock zone. The average profile 1 is applied between 168 bpm and the lower limit of the conditional shock zone during acceleration and between the lower limit of the conditional zone and 148 bpm during deceleration. The second plateau varies depending on the comparative analysis of the amplitude of the two previous QRS complexes (judged to be similar or different). Average profile 2 is applied in the conditional shock zone. For example, if a conditional shock zone is programmed at 180 bpm with a shock zone at 230 bpm, profile 1 is applied between 168 and 180 bpm and then between 180 and 148 bpm. The average profile 2 is applied between 180 and 230 bpm.
- Slow profile: this profile is suitable for the slowest frequencies (<168 bpm during acceleration and <148 bpm during deceleration). The main objective in this zone is to reduce the risk of T wave oversensing. There are therefore two different slow profiles depending on whether or not there is a difference in amplitude between the two previous complexes (suspected T wave oversensing).
The difficulty lies in determining the duration of ventricular arrhythmia beyond which the delay in delivering an electric shock is too long, especially since subcutaneous defibrillators are mainly indicated in patients who are more likely to experience episodes of malignant arrhythmia such as VF rather than monomorphic VT. For VF lasting more than 20 seconds, syncope is certain to occur, and older studies have found an increased risk of ineffective therapies. The only possibility for reprogramming today is to change the vector, with no guarantee that a second vector will provide improved detection.
Counters during charging
Once started, capacitor charging continues until the device reaches its target voltage, at which point reconfirmation is applied to verify that the arrhythmia is continuing and that there has been no spontaneous reduction. At the start of capacitor charging, two counters are opened:
- a consecutive fast cycle counter (SC Fast Intvls) which is incremented by consecutive fast raw intervals (“•” and “N” included if the raw interval is short) and not according to the S or T classification; this counter resets to zero as soon as a long raw interval is detected; during charging, a long interval (if the conditional shock zone is programmed to 200 bpm, an interval is long if it exceeds 300 ms) therefore resets this counter to 0.
- a counter of consecutive fast cycles required to deliver the shock (SC value): it starts at 3 and cannot fall below 3; a minimum of 3 consecutive fast cycles at the end of charging is therefore required to deliver the shock; this counter is incremented by each slow cycle classified as S (+1) and decremented by each fast cycle classified as T (-1, minimum value: 3); this counter is therefore not based on raw intervals like the previous one.
- At the end of charging, the shock can be delivered when SC Fast Intvls ≥ SC value. This algorithm allows continuous rhythm analysis during capacitor charging without deviating from the charge. In fact, once charging begins, it cannot be interrupted.
The charge is diverted if the average 4 RR interval is greater than the lowest frequency zone + 40 ms for 24 intervals. An untreated episode is then recorded in the memory and the initial persistence is extended by 3 cycles as explained above (Smart Charge).
At the end of the charge, there is always a second C marker corresponding to the “top-off charge.” On telemedicine tracings, the end-of-charge markers are also visible. The first charge brings the device close to the 80 joules that must be delivered. The second charge completes and adjusts the amplitude of the shock delivered to exactly 80 joules. When this second C marker appears, the shock is “committed” and delivered. One or two S markers (last cycle before the C marker) may then appear on the trace even if the frequency corresponds to a tachycardia zone, as the device stops its analysis.