False diagnosis of tachycardia due to an oversensing issue
Tracing
Manufacturer Biotronik
Device ILR
Field Biomonitor
N° 9
Patient
90-year-old woman participating in the LBBB-TAVI study.
Graph and trace
Tracing 9a: episode diagnosed as HVR;
- well sensed QRS complex;
- T wave oversensing;
- diagnosis of HVR by the device in conjunction with this systematic T wave oversensing.
Patient: 85-year-old woman participating in the LBBB-TAVI study.
Tracing 9b: episode diagnosed as HVR;
- railroad track pattern of the tachogram evoked by the oversensing of a physiological signal (P wave, T wave, double counting of the R wave);
- well sensed QRS complex;
- P wave oversensing;
- diagnosis of HRV by the device in conjunction with this systematic P wave oversensing.
Patient: 92-year-old woman participating in the LBBB-TAVI study.
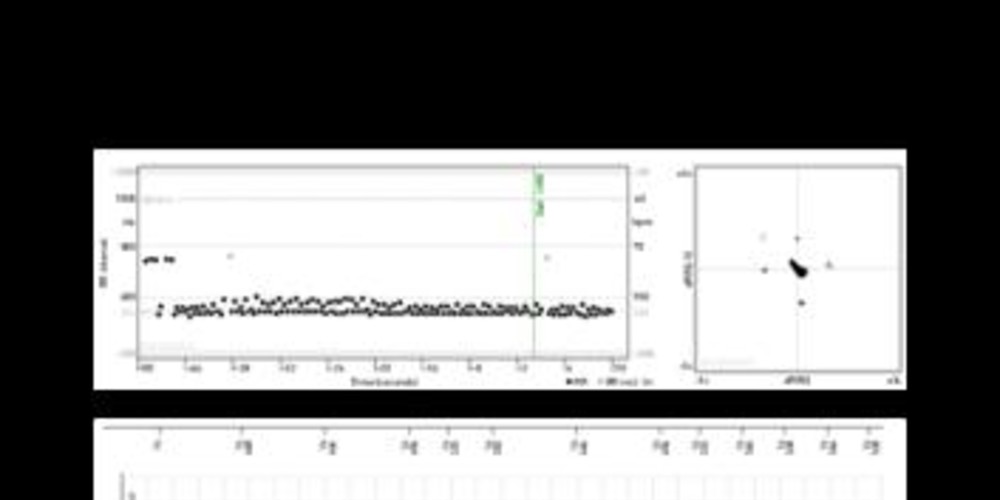
Tracing 9c: episode diagnosed as HVR;
- noise interference of the baseline with intervals classified as Vn;
- tracing slightly less artifactual with intervals classified as Vs which leads to the diagnosis of HVR.
Other articles that may be of interest to you




To avoid the recording of multiple episodes of false tachycardias saturating the memory bank, two options are preferred: 1) at the time of implantation, it is important to optimize the positioning of the device in order to obtain ventriculograms of sufficient amplitude without significant variation between intervals. Likewise, it is important to adjust the size of the subcutaneous pocket in order to reduce movement of the device and to avoid the oversensing of noise artifacts; 2) optimization of the programming can reduce the risk of oversensing of the P wave, the T wave and the double counting of the R wave.
The first patient presented T wave oversensing and multiple false diagnoses of HVR recorded in memory. T wave oversensing is favored by a decrease in R wave amplitude. Indeed, the sensing threshold is adjusted as a function of the amplitude of the previous R wave. For a T wave of similar size, the oversensing is thus all the more likely if the previous R wave is of small amplitude. In this example, the amplitude of the R wave is appropriate; on the other hand, the T wave is of high amplitude leading to oversensing. To correct the problem, it is possible to program the T wave suppression option with modification of the filters (elimination of low frequency signals) as well as the initial threshold (100% in order to reduce sensitivity at the beginning of the cycle) and the threshold target.
The second patient presented P wave oversensing, with a characteristic railroad track pattern on the tachogram (alternation between 2 intervals) observed during the sensing of an additional cardiac signal (double counting of the R wave; P wave or T wave oversensing).
For the last patient, the diagnosis of noise is obvious and initially correctly diagnosed by the device. The device classifies a sensed interval as noise under 2 conditions: 1) when the signal is of too weak amplitude (small signals); signals < 44μV are never sensed (maximum sensing capacity of the device); signals with an amplitude between 44 and 88μV are considered as low amplitude and are classified as Vn in order to avoid oversensing and improve specificity; 2) when the signal is of too high frequency (very rapid signals); following the sensing of a signal, there is a noise window to prevent oversensing of non-physiological signals; when a signal is sensed in the noise window, it is classified as Vn; when the noise is continuous, a Vn marker appears on the marker chain every 200 ms; it is possible to prolong this window with a risk of undersensing of a fast ventricular rhythm.
The sensing of intervals classified as Vn interferes with the various counters. Vs/Vn intervals are never integrated in the arrhythmia count. The HVR and the drop in rate counters are systematically reset to 0 after each interval classified as Vn. If the noise counter exceeds 25% (at least 1 interval out of 4 classified as Vn) on 2 consecutive windows, the sensing and confirmation of the AF are canceled.