False diagnosis of bradycardia or asystole due to sensing failure
Tracing
Manufacturer Biotronik
Device ILR
Field Biomonitor
N° 8
Patient
70-year-old woman participating in the LBBB-TAVI study; asymptomatic.
Graph and trace
Tracing 8a: episode diagnosed as asystole;
- stable ventricular rhythm; atrial activity difficult to discern;
- marked undersensing of the QRS complexes in conjunction with a progressive decrease in signal amplitude;
- diagnosis of asystole by the device in conjunction with this undersensing.
Patient: 82-year-old man participating in the LBBB-TAVI study.
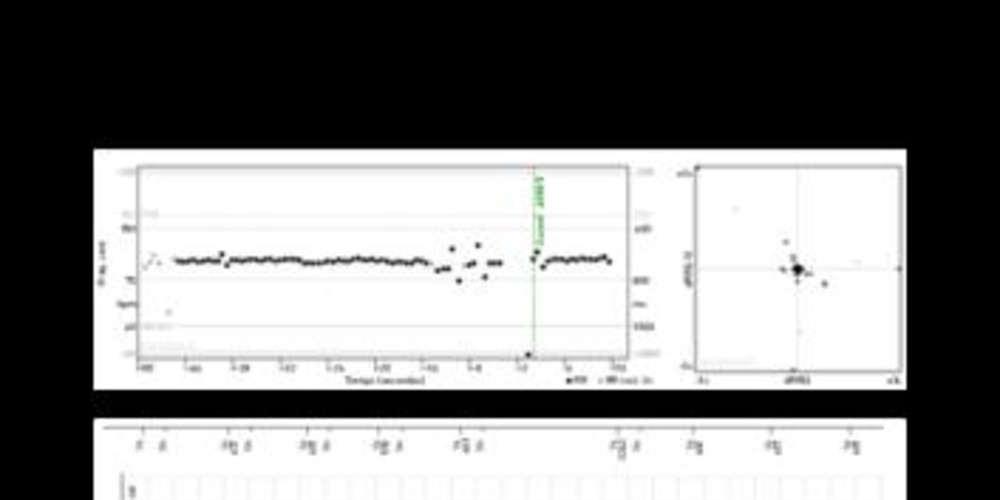
Tracing 8b: episode diagnosed as bradycardia;
- characteristic pattern (tachogram, Lorenz plot, ECG tracing) of PVC with premature complex followed by compensatory pause;
- undersensing of sinus complexes following the PVC;
- bradycardia diagnosis by the device in conjunction with this undersensing.
Patient: 82-year-old man participating in the LBBB-TAVI study.
Tracing 8c: diagnosed episode as bradycardia;
- sinus rhythm correctly sensed;
- likely PVC not sensed by the device;
- diagnosis of bradycardia by the device in conjunction with this undersensing together with the compensatory pause following the PVC.
Other articles that may be of interest to you




The automatic recording of episodes of bradycardia or tachycardia allows increasing the diagnostic yield of the implantable loop recorder. The asymptomatic and symptomatic episodes in patients occurring in patients without the ability to actively trigger the recording are thus memorized. However, an important limitation of this function is the frequent spurious recording of false arrhythmias such as bradycardia due to undersensing of ventricular signals or tachycardia due to sensing of noise or other intra-cardiac signals such as P waves or T waves or double counting of the R wave. This implies that all the episodes stored in the memory need to be verified. The recording of spurious arrhythmia episodes is frequent since found in over half of the implanted patients.
It is possible to modify the programming in order to avoid the iterative recording of false bradycardia episodes. Four programming options are available with different filter and target threshold values (standard, variable amplitude, T wave suppression, premature ventricular contraction detection):