Tachycardia and zones
Patient
A 56-year-old ischemic patient, with ejection fraction of 30% and symptoms of heart failure, implanted with an atrio-biventricular defibrillator (narrow QRS but with frequent episodes of Mobitz I second-degree AV block).
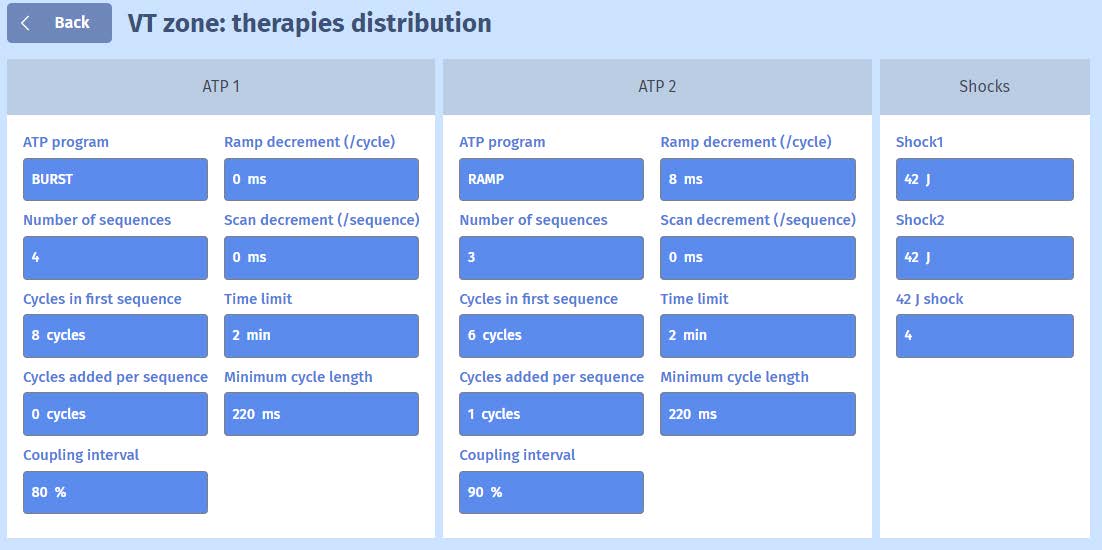
Programming

EGM
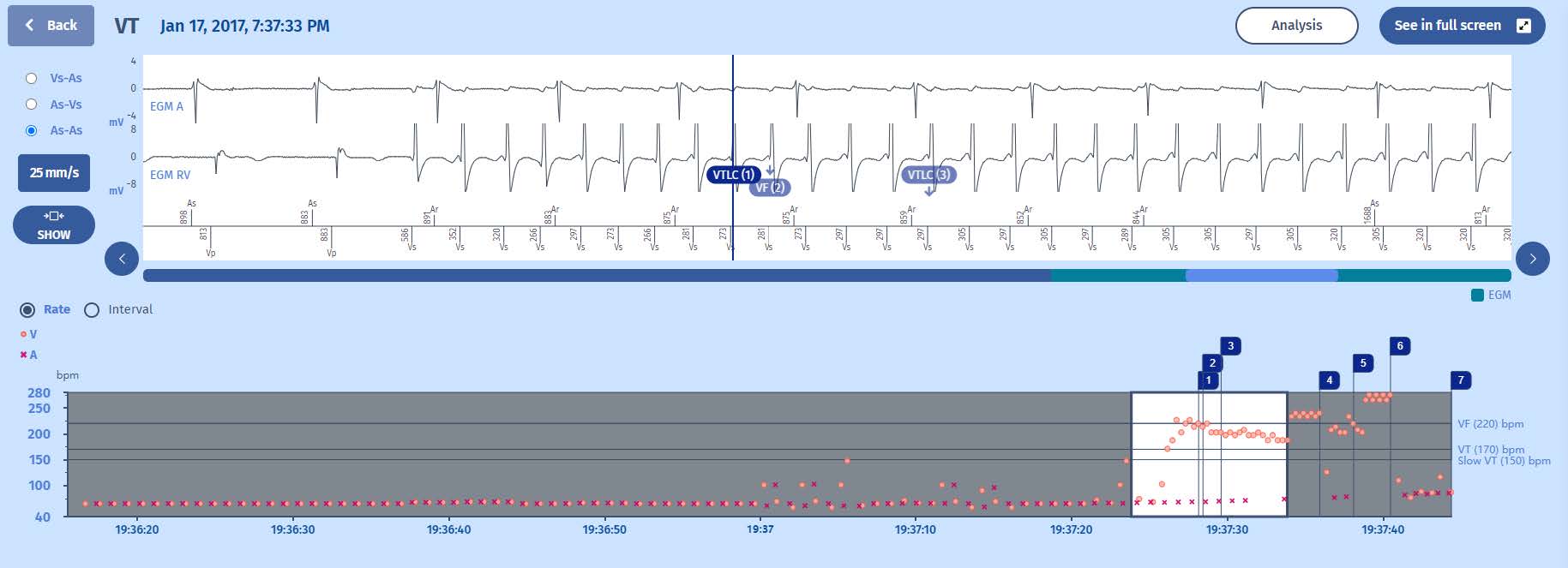
Interval plot
1 The rhythm is initially sinus, then appearance of premature contractions and the tachycardia begins
2 The tachycardia is in the VT zone, bordering on the FV zone,
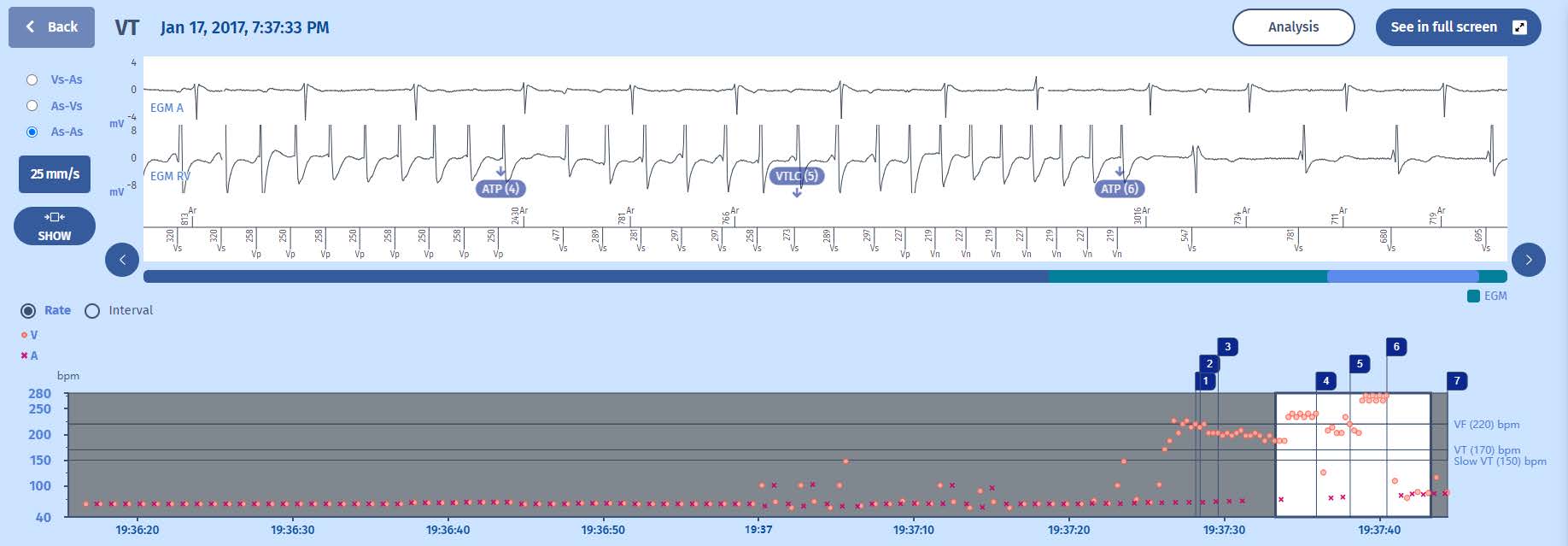
3 And an ATP burst is applied which leads to an acceleration of the tachycardia, which nonetheless remains in the VT zone
4 And at the end of redetection, a second faster burst terminates the tachycardia

EGM
- A monomorphic ventricular tachycardia begins abruptly with atrial dissociation
- Ventricular far-field signals are visible on the atrial EGM, but are not detected
- After excluding the first two tachycardia cycles in the VT zone, the following 6 cycles lead to a first VT diagnosis.
- There is a gradual acceleration at the onset of the tachycardia such that the diagnosis is quickly VF
- The tachycardia then stabilizes with a slight deceleration leading again to the diagnosis
of VT
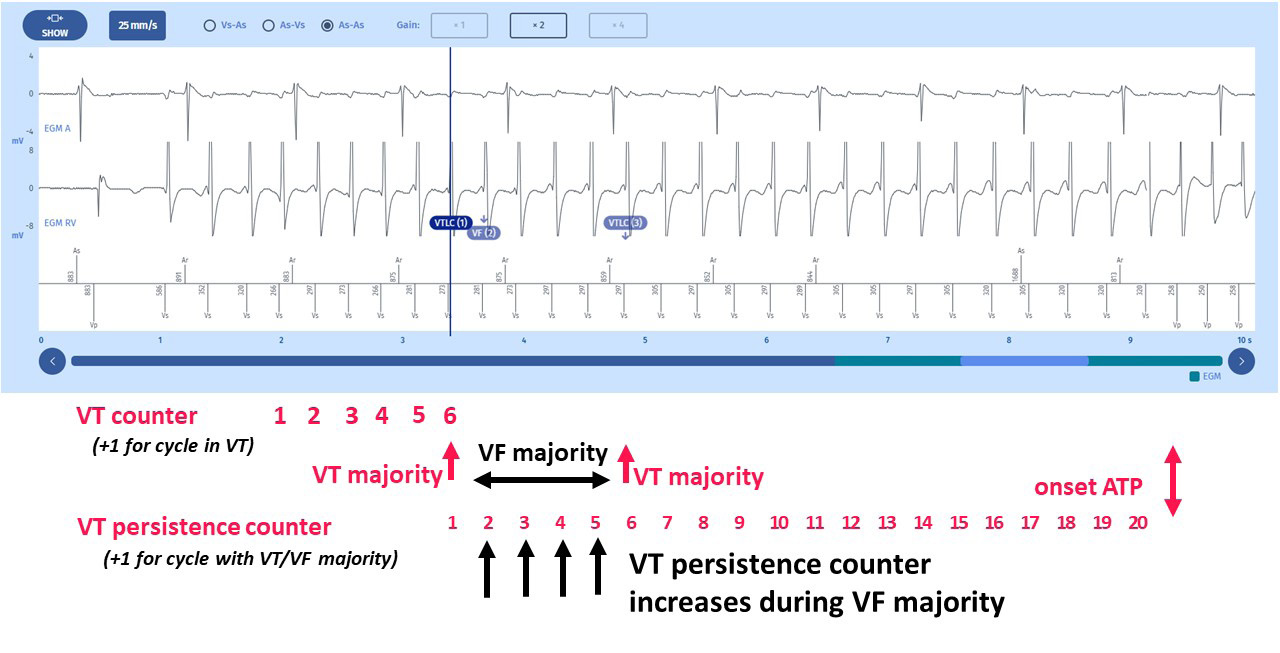
- From the first VT diagnosis (1st VTLC annotation noted on the tracing), the VT counter is incremented at each cycle, each validating the VT diagnosis. The VT persistence counter of 20 cycles (as programmed for this zone) therefore begins
- During the short time period where the tachycardia is noted VF, the VT counter continues to increment and VF counter starts to increment.
- The second VTLC annotation interrupts the VF counter, but continues to increment the VT counter until reaching the number of 20, which triggers the first therapy in the VT zone, a burst of 8 cycles with a coupling interval at 80% of the average of the last 4 persistence cycles (320 ms)
- The ATP does not terminate the tachycardia which is even faster than before the ATP
- After the ATP, the tachycardia continues. The 1st cycle post-ATP is not taken into account, and during the redetection cycles, the diagnosis of VT is obtained, and the second therapy of the VT zone is applied with a pacing coupling time of 80% of the
average of the last 4 cycles of the redetection phase (281 ms)
- The cycles of this second ATP have a coupling interval at the limit of the minimum allowed coupling of 220 ms.
- This burst terminates the tachycardia
Comments
- This case illustrates the counting of cycles during the tachycardia with an increment of the VT counter when the cycles are labelled VF majority, with again, the risk of acceleration of the VT by the therapies. Here, the consequences are modest since the
tachycardia is accelerating, obviously, but is quickly terminated by the next burst.
- The ATP coupling interval adjusts itself to the tachycardia rate which initiates the therapy. Each ATP will therefore have a rate depending on the average of the last 4 VT cycles prior to therapy.
- The ATP rate, whether it is a burst or a ramp, cannot be faster than the programmed minimum cycle length, in this instance 220 ms.
- A comment on the programming of the prosthesis. We can see that two types of therapies are programmed in the VT zone: bursts followed by ramps. We also note that no pacing cycle is added to each burst, while a cycle is added to each ramp. This
means that the first ramp has 6 pacing cycles, the second has 6+1 cycles, the third 7+1 cycles, and so forth. This results in an increased aggressiveness of the ramps, whichcan cause acceleration, or the triggering of a VF thus necessitating a shock. It is better to increase the number of burst cycles rather than the number of ramp cycles.
Take home message
The ATP pacing rate is dependent on the average tachycardia rate prior to their delivery.
If successive therapies modify the tachycardia, the ATP rate adjusts itself to these changes.

