Extracardiac oversensing
Patient
In this example, the patient was recently implanted in primary prevention for obstructive hypertrophic heart disease. He experienced a sudden syncope, has a family history of
sudden death (father and brother), a subaortic obstruction measured at 74 mmHg at rest and 120 mmHg at exercise, a septal thickness of 24 mm, no ventricular bursts on Holter
monitoring, but a significant septal fibrosis on MRI. A genetic study is in progress. Given the above, the patient received a dual-chamber system in an attempt to reduce subaortic obstruction while simultaneously protecting against ventricular arrhythmia disorders. The right ventricular lead was thus placed at the apex of the RV, with continuous pacing by the device to reverse the ventricular activation sequence and minimise the obstruction on ejection. The pre-discharge follow-up control is quite satisfactory as well as the chest radiograph. We quickly receive a telemedicine alert because the patient received a maximal shock for VF. The patient is recalled immediately for consultation. No symptoms occurred prior the
shock which surprised the patient while attempting to retrieve an object that had slipped under the seat of his car! The leads work perfectly.
Programming
A VT zone is programmed starting at 180/min with a persistence of 12 cycles and a VF zone starting at 230/min with a fast VT section of 230 to 255/min with a burst followed by shocks, and
a VF section with maximum shock directly.

Interpretation
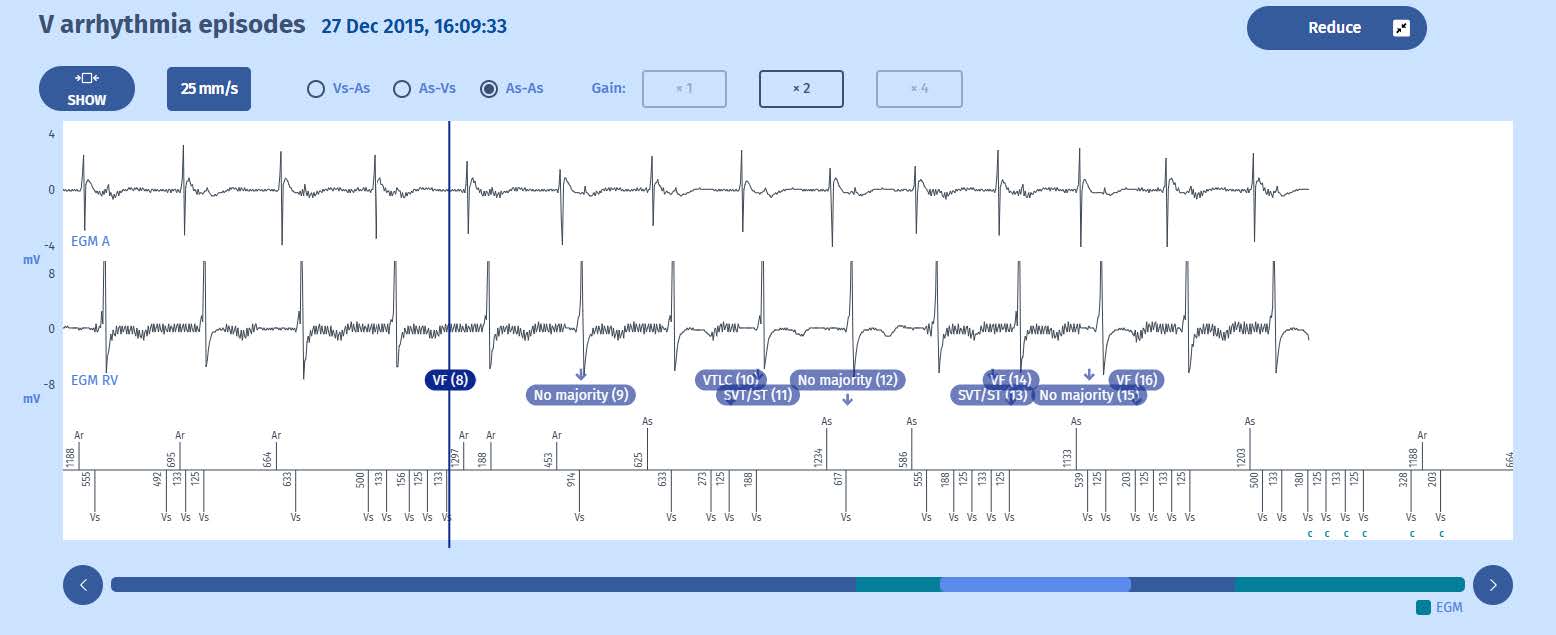
- Using the EGM « Zoom » function to amplify and expand the tracing make EGMs much easier to interpret.
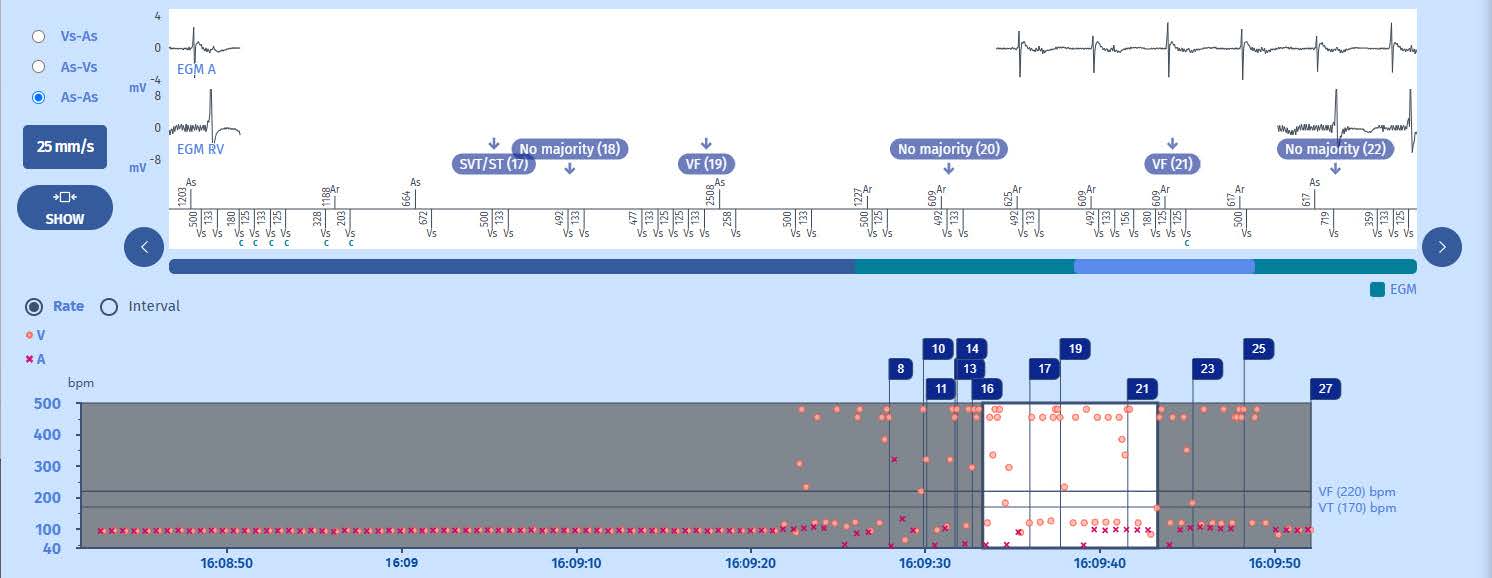
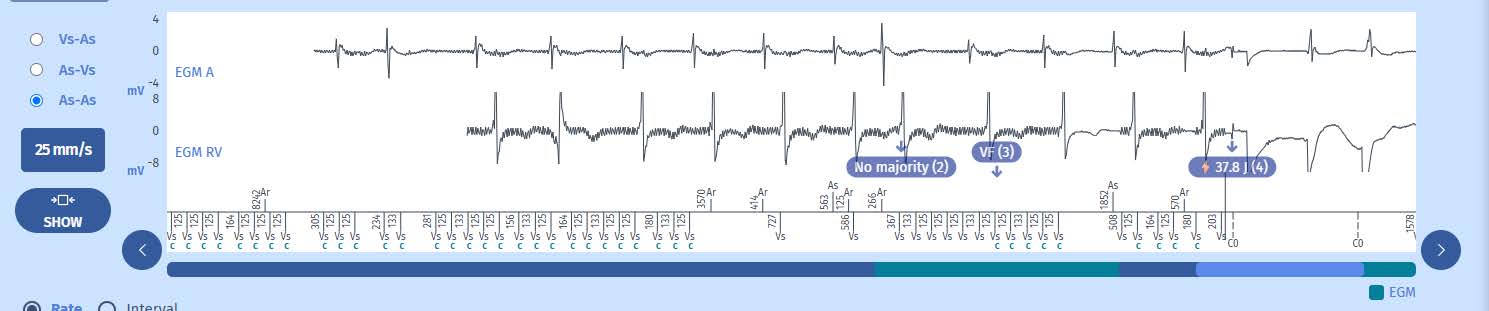
- It is clear that the ventricular detections with very short RR intervals do not correspond to any ventriculogram on the ventricular EGM. It is therefore oversensing.
- Many RR intervals have a duration of 125 ms which is the value of the post-ventricular ventricular blanking. Such values are not physiological but correspond either to external interference, a 50 Hz current, myopotentials, a lead facture, or a connection fault.
- Analysis of the morphology of the oversensing on the EGM is therefore essential. Byexpanding the Case, we see that the line is thick on the ventricular EGM, but also to a certain degree on the atrial signal. This phenomenon can correspond to an external interference, a 50 Hz current, diaphragmatic-type myopotentials, although likely not pectoral, but certainly not to a lead fracture or a lack of connection which would cause chaotic potentials of large amplitude. In addition, the manipulation of the defibrillator case through the skin, which could not be aggressive given the very recent implantation procedure, does not induce any aberrant signal on the EGM in real-time. The circumstances surrounding of occurrence of the shock do not evoke exposure to external interference or a 50 Hz current. Hence, myopotentials? Counter movements of the arm, which are also painful, do not give rise to any anomaly.
- On the other hand, the intermittent and sometimes regular nature of the appearance of the aberrant signals and the reproduction of the phenomenon on both leads
through deep breathing during the consultation signal the diagnosis of myopotentials of diaphragmatic origin! A control image reveals that the ventricular lead is in its
proper position, placed along the anterior aspect of the RV, while the atrial lead has moved to the anterior and lateral side of the RA, next to the right hemidiaphragm!
Hence the reason for the observed artefacts in the form of a thick line appearing on the atrial EGM when the patient performs deep respiratory movements, an event
reproducible in consultation. The atrial signals are, however, not of sufficient amplitude to be detected.
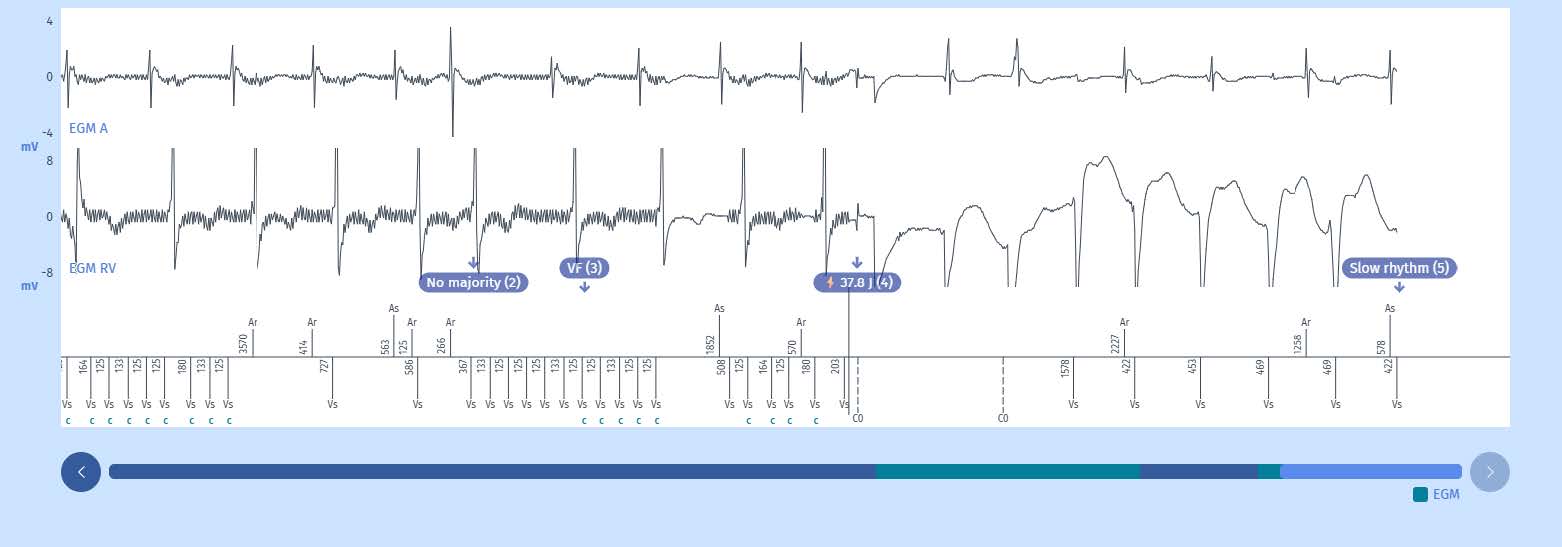
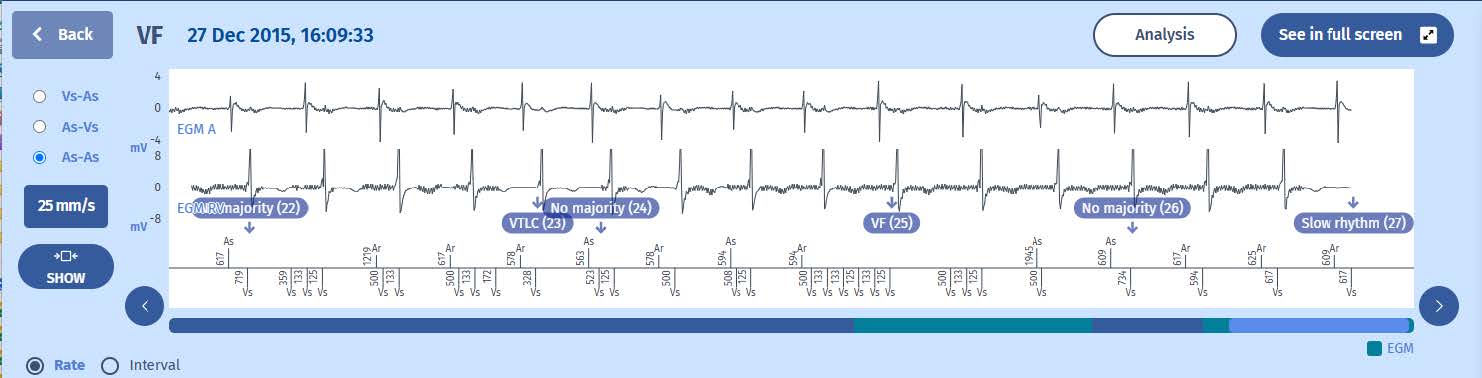
6. We can also observe that the charging of the capacitors was not homogeneous, the process being interrupting upon the appearance of slow cycles causing the absence of majority. The charging of the capacitors resumes as soon as the majority becomes VF again. At the end of the charge, the next cycle being in the VF zone, the shock is delivered. However, in this instance, a slow ventricular tachycardia was induced, detected outside of the VT or VF zone, such that the episode terminates due to the diagnosis of « Slow Rhythm », while the tachycardia continues. We do not know how long the latter persisted. The patient states he remained asymptomatic.
Take home message
When extrinsic oversensing is suspected, it is imperative to thoroughly analyse the entire EGM in order to characterise the signals as well as perform systematic provocative manoeuvres
in concomitance with the analysis of the cardiac signal in real time by the programmer in the “EGM” test screen. The interview of the patient is essential to identify the situation at the
origin of this oversensing. The use of the RF communication function facilitates these tests by eliminating the programming head.
Finally, if the phenomenon is observed within the first few days or weeks after implantation, a connection problem should be suspected. However, after several months or years, this latter
hypothesis is no longer plausible.

