A well classified 1:1 tachycardia
Patient
A 65-year-old man implanted with an INTENSIA DR dual-chamber defibrillator in secondary prevention for post-infarction dilated ischemic heart disease with highly altered ejection fraction, stage III heart failure and narrow QRS.
Programming
3 zones with :
1 A Slow zone starting at 125/min, 30 persistence cycles, with ATP and shock sequences
2 A VT zone starting at 185/min
3 A VF zone starting at 240/min
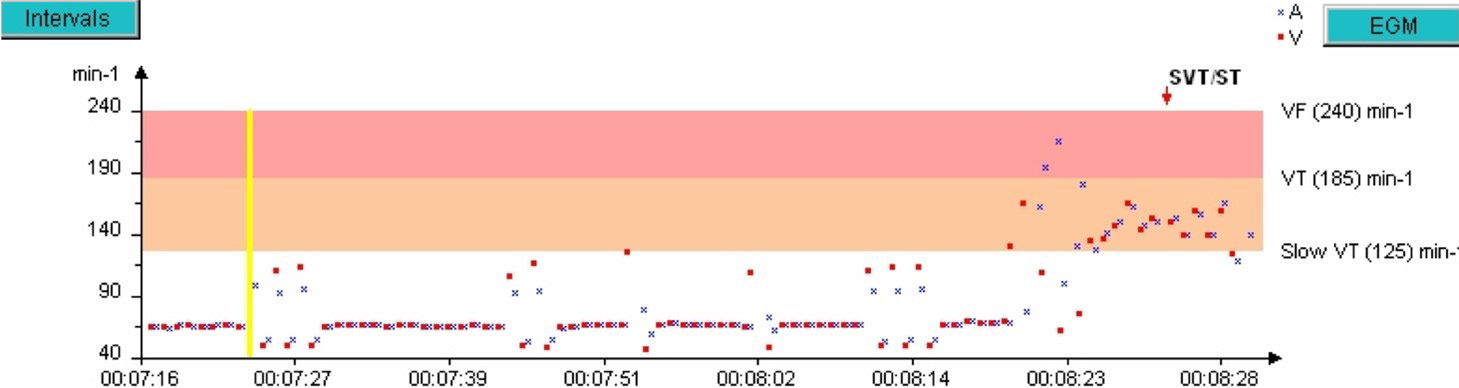
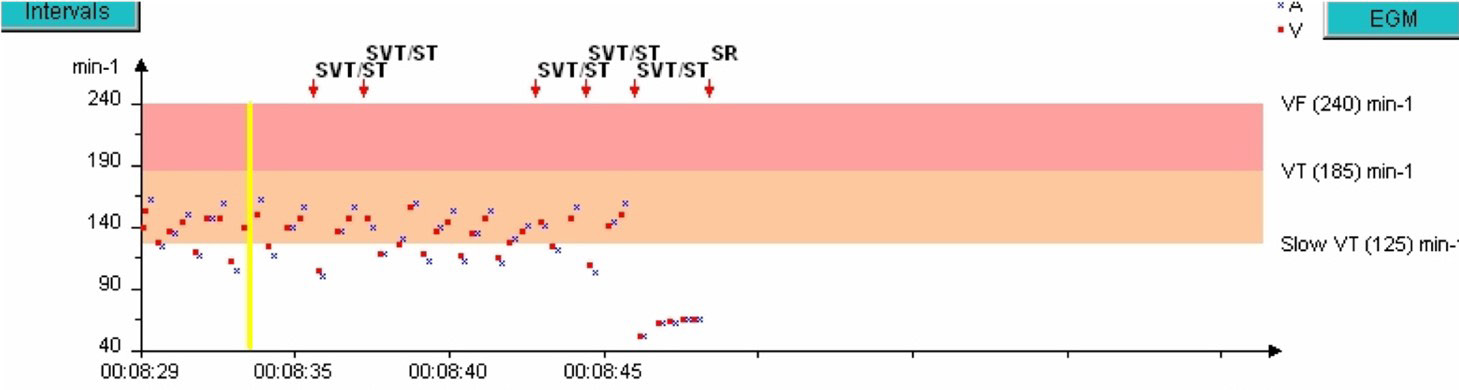
Rate interval plot
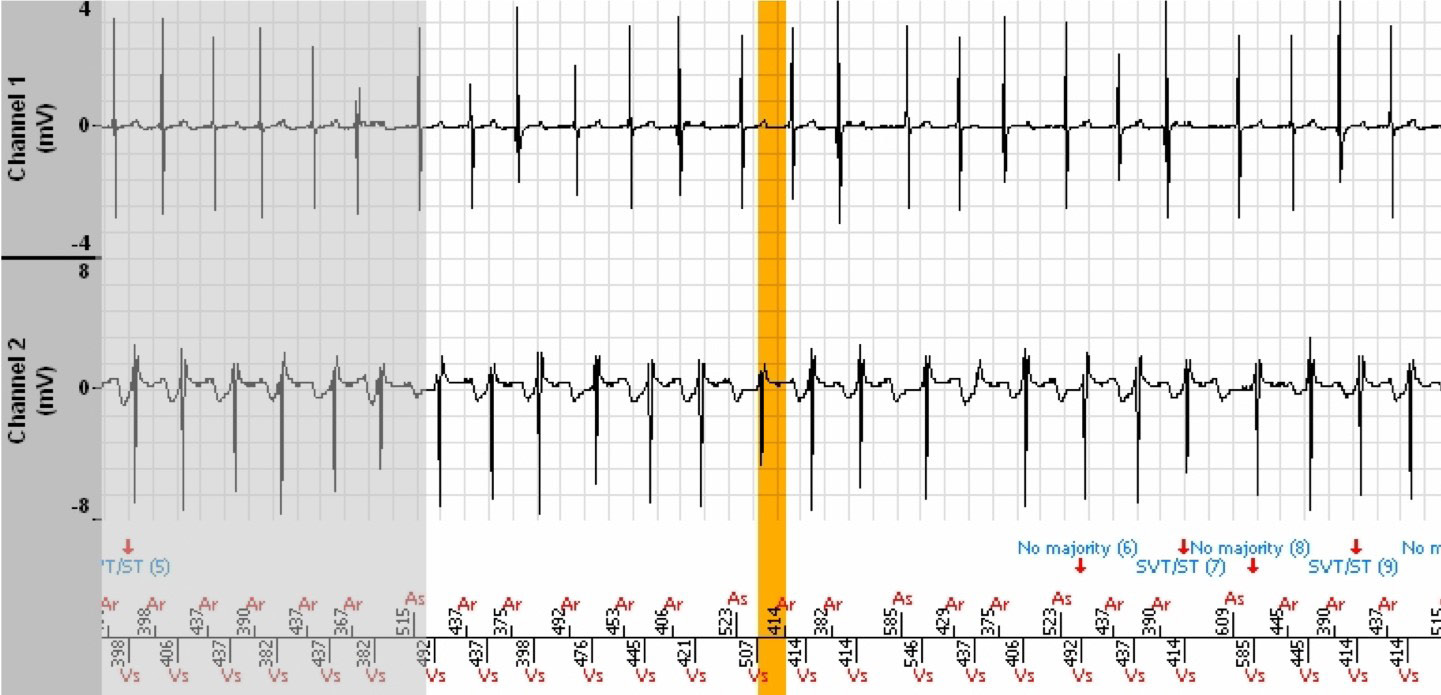
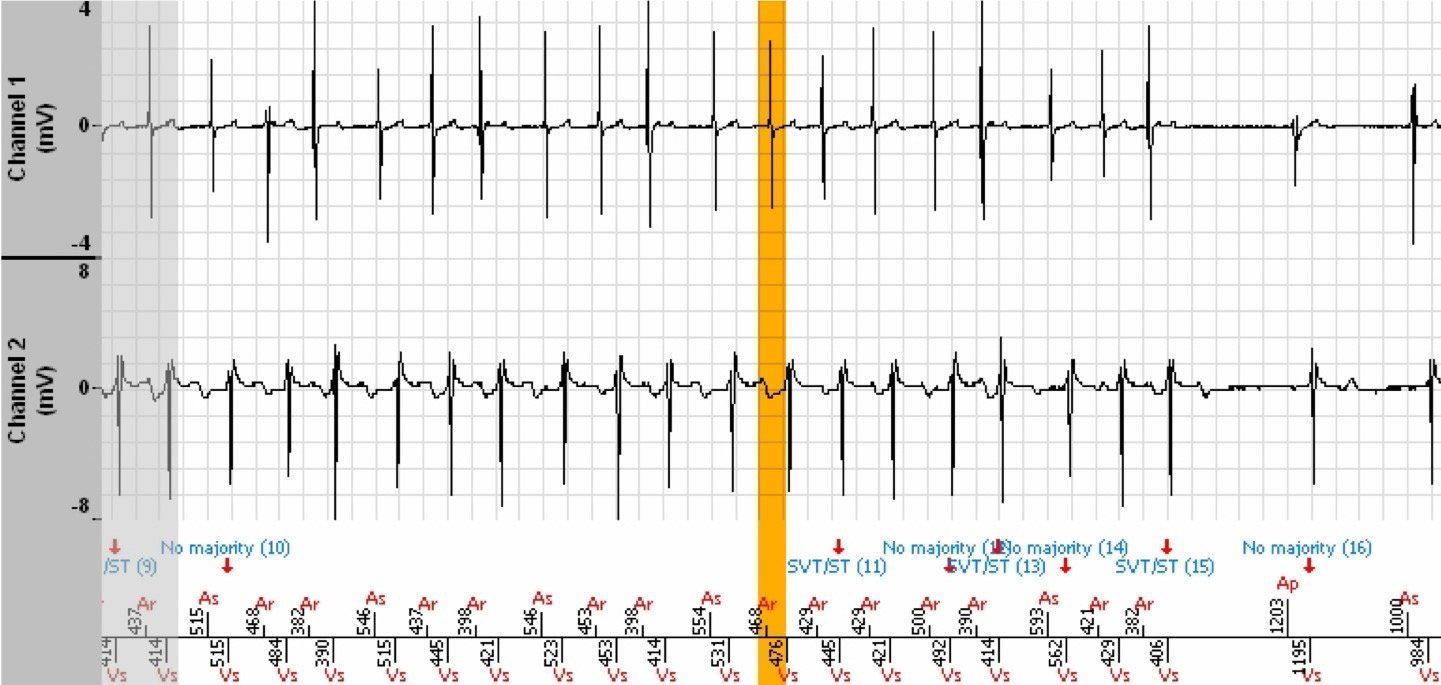
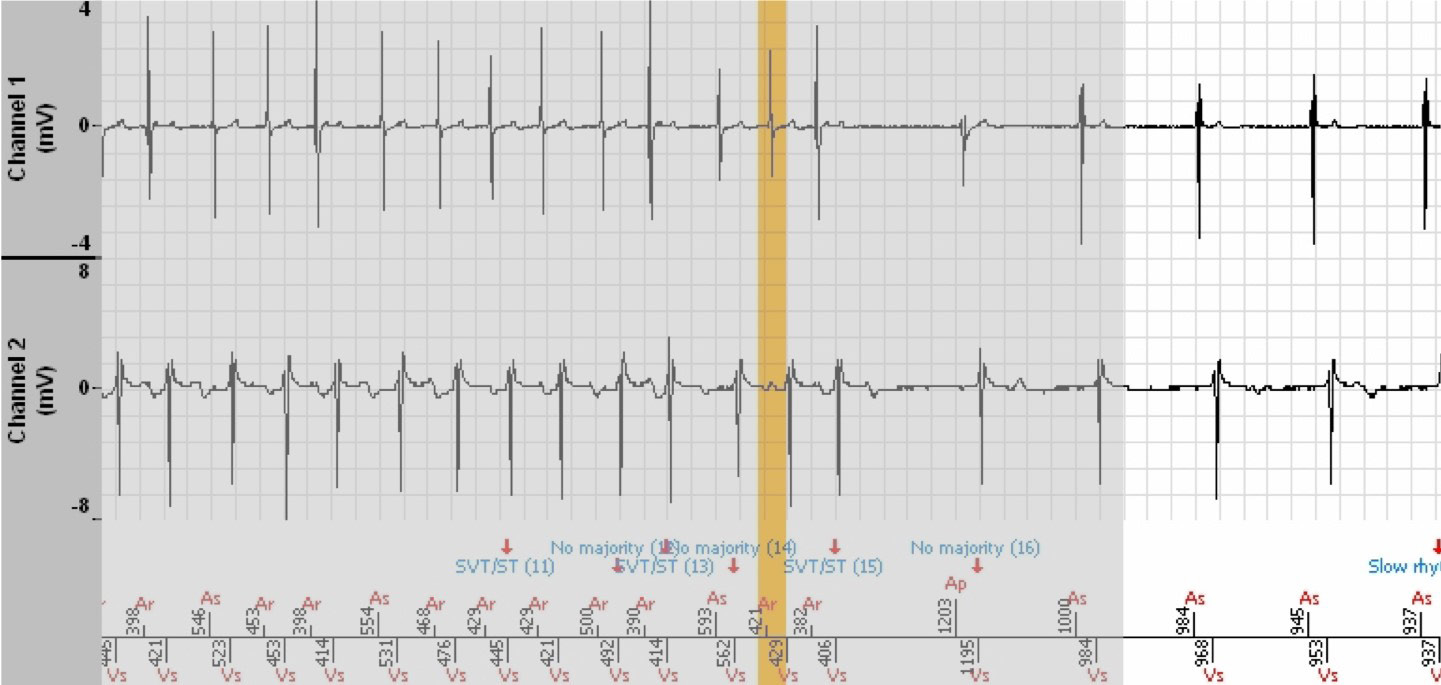
EGM
The shaded areas are the portions of the EGM that are the repetitions of the end of the previous image.

Interpretation
- The tachogram reveals both atrial and ventricular premature contractions during conducted sinus rhythm.
- The tachycardia is preceded by a ventricular triplet with probable retrograde conduction, followed by an immediate destabilisation of the atrial rhythm which initiates an unstable atrial tachycardia and reflected in the ventricle, leading to the
diagnosis is SVT. Each variation of the P’P’ interval induces the same variation of the corresponding RR interval. The tachycardia is well controlled by the atrium.
- The diagnosis is No majority when the rhythm enters or returns in the Slow zone (non Tachy) for at least 3 out of 8 cycles (but less than 6), then again becomes unstable with a diagnosis of SVT until termination of the episode.
- No therapy was induced.
Comments
- The rhythm is viewed as stable, 1:1, with A acceleration, hence the diagnosis of SVT.
- Of note: the atrial markers are either As or Ar during the entire episode. This signifies that the defibrillator is constantly suspicious of atrial arrhythmia identified by the Fallback Mode Switch algorithm that functions in parallel. The As markers appear when
the Ar-As interval is greater than 500 ms. This is not specific to the defibrillator, but to the Fallback Mode Switch algorithm of all platforms of the brand, both pacemakers and defibrillators.
Take home message
The dual-chamber defibrillator primarily classifies tachycardias in the same manner as a single-chamber defibrillator, taking into account stability as first line analysis. In the absence of a morphology algorithm, the quality of the diagnoses is highly dependent on the quality of atrial sensing that is itself dependent on the atrial lead and the ability of the defibrillator to detect P waves outside of the refractory periods, hence highlighting the care duly required at the time of implantation of this atrial lead.

