You interrogate the device

This is the newest episode
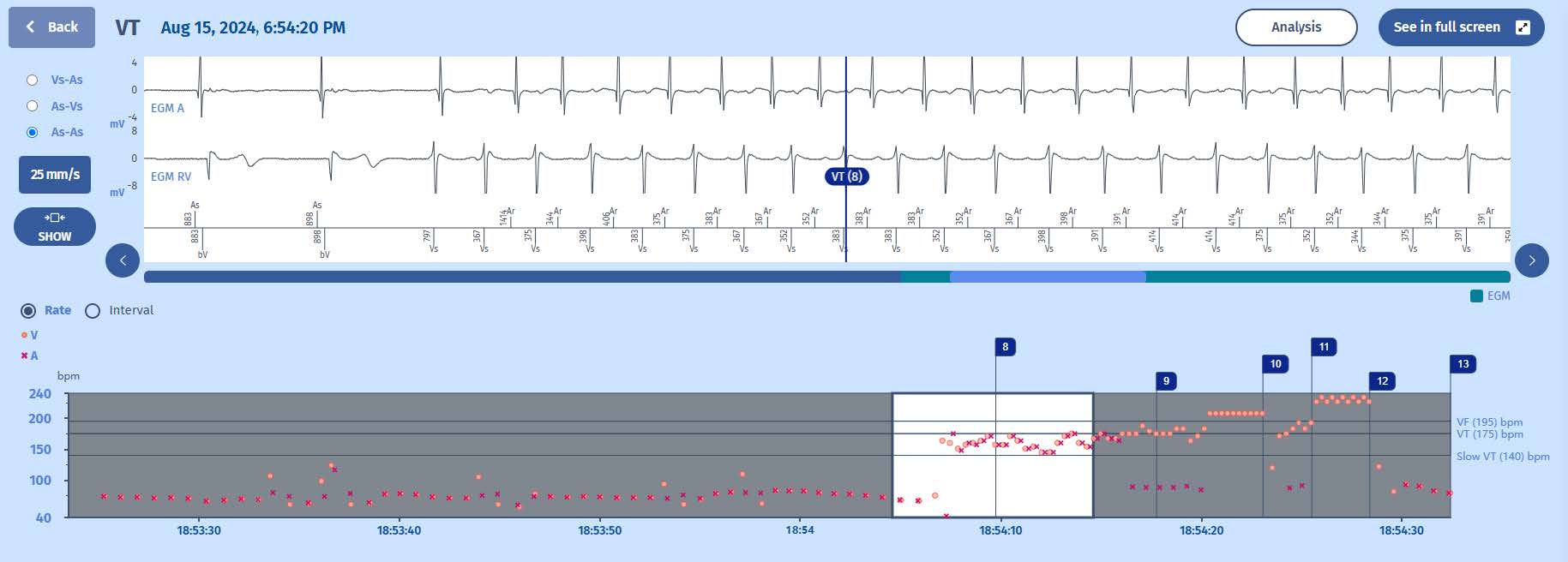
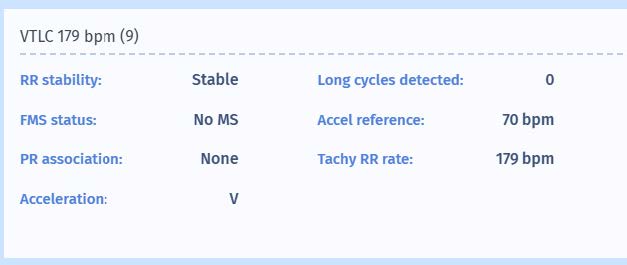
When we look closely at the onset of the arrhythmia, we can see that the first chamber to accelerate is the ventricle, driving the atrium. We can see that after 6 events in the VT zone (after discarding the initial two events from the RR stability, PR association and level of PR association criteria), the diagnosis of VT is made. Please note that the marker is VT, and not VTLC. This means that the tachycardia has followed another path in the decision tree than the previous cases. When we analyze the VT marker, we can see that the arrhythmia is indeed stable, but that because of PR association, the PARAD+ algorithm continues to look for criteria. There is 1:1 association according to the PARAD+ algorithm and therefore it proceeds to the next step. This is a check whether the
acceleration is sudden, because sinus tachycardia is a stable tachycardia with 1:1 PR association and this needs to be excluded to diminish the risk of inappropriate therapies. In this case, the onset is sudden with an acceleration from 70 bpm (reference) to 163 bpm (tachy RR rate). When sinus tachycardia has been excluded, there is a last step. Which is exclusion of atrial tachycardia; a tachycardia with sudden onset, is stable, is associated in a 1:1 fashion. The best way to exclude atrial tachycardia is to analyze which chamber was first to accelerate. For atrial tachycardia this will be the atrium. For ventricular tachycardia, the first chamber to accelerate is the ventricle. In this case, the ventricle has been correctly identified as the first chamber to accelerate.
Therefore, the diagnosis is VT. Mentioned information is all displayed in the analysis figure below.
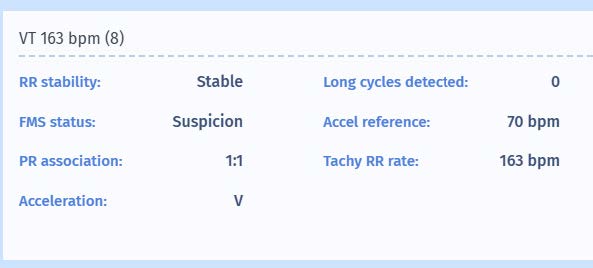
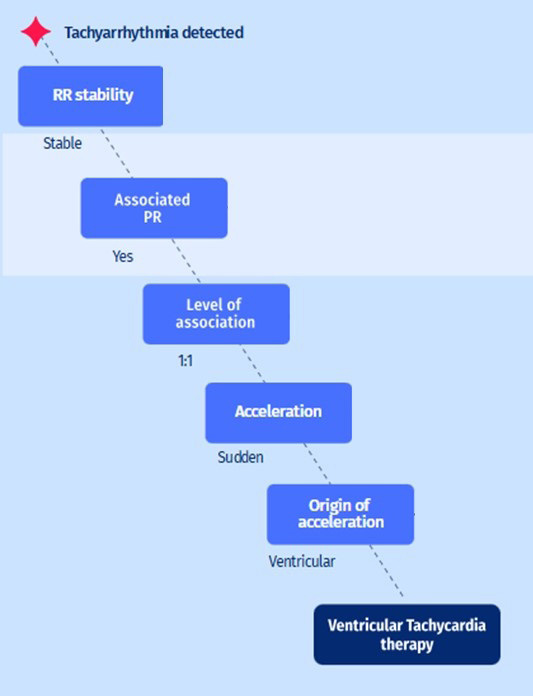
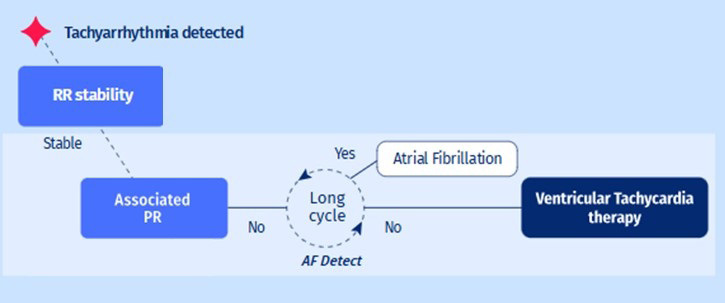
Illustration of the decision tree (PARAD+) of the beginning of the EGM:
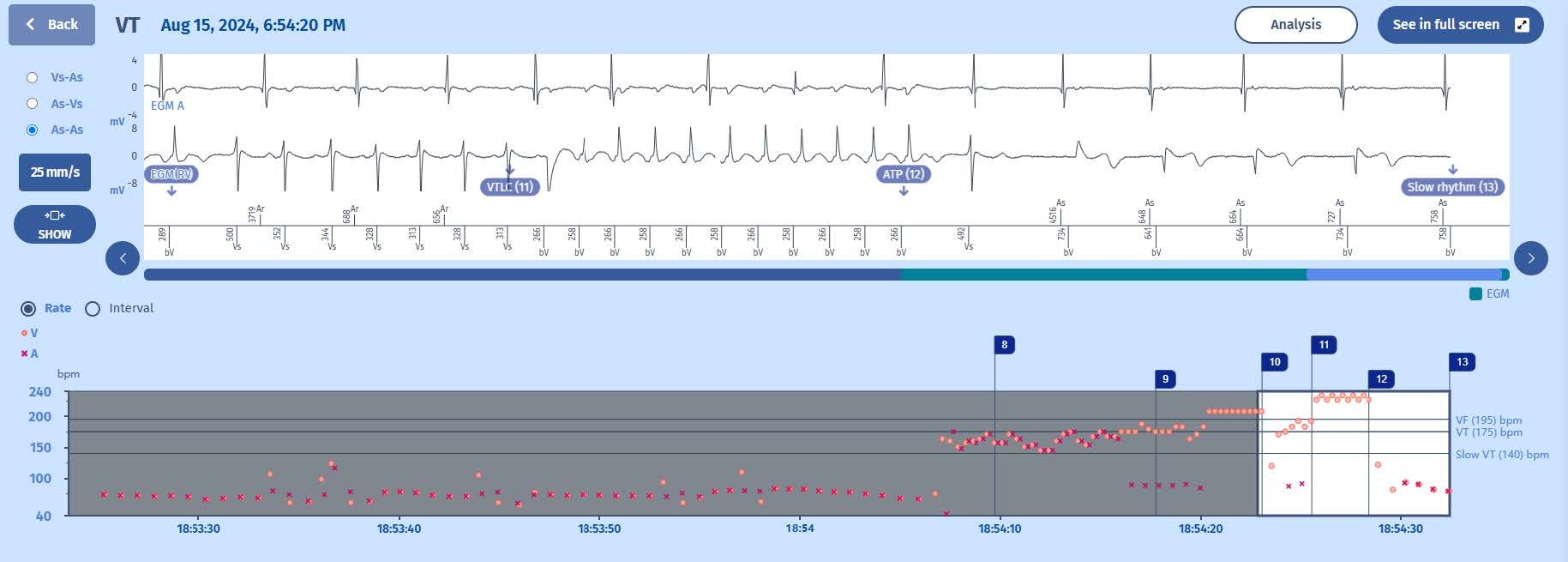
The continuation of the EGM:
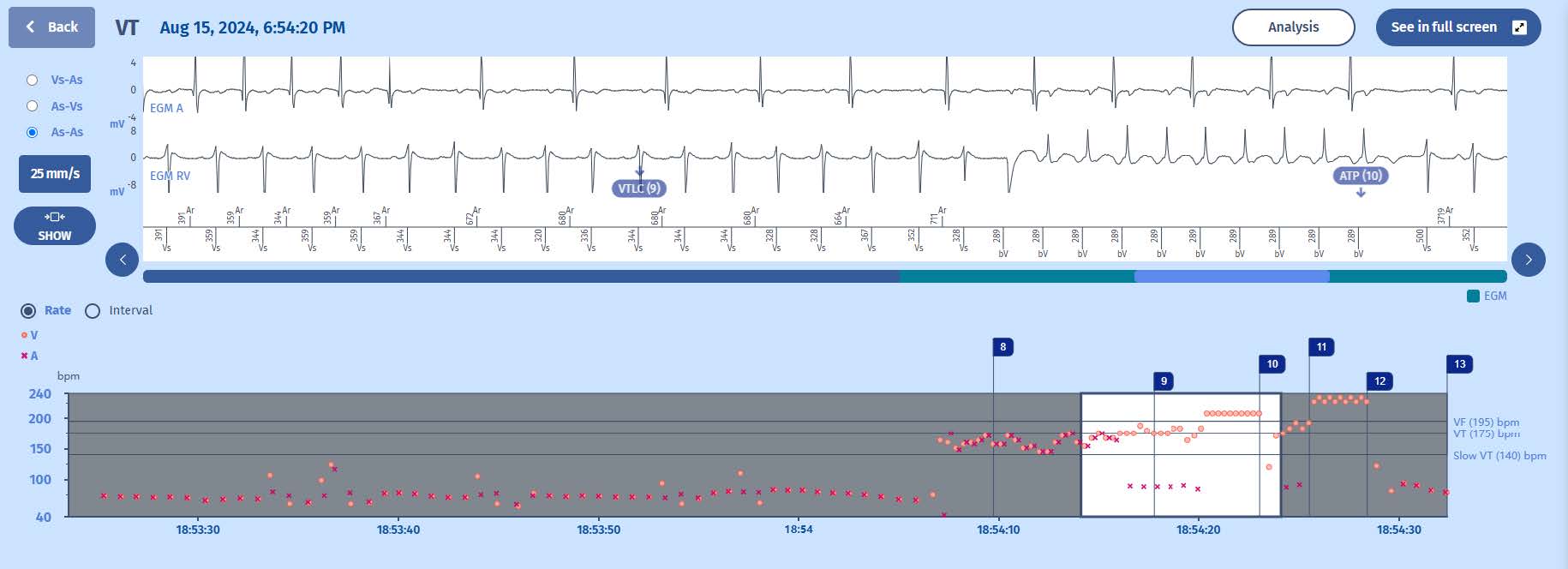
Notice how the marker changes from VT to VTLC. This is because the decision tree of the PARAD+ has changed. The retrograde (VA) conduction has diminished to a 2-to-1 fashion with loss of PR association. Therefore, the discrimination goes back to checking whether the ventricular rate is stable and VT is diagnosed. Again, the analysis button may help to better understand the PARAD+ algorithm, as it will display that the PR association is lost (“none”).
Therefore, we may illustrate the decision tree (PARAD+) of the second part of the EGM like so:
The continuation of the EGM: