


Trace description
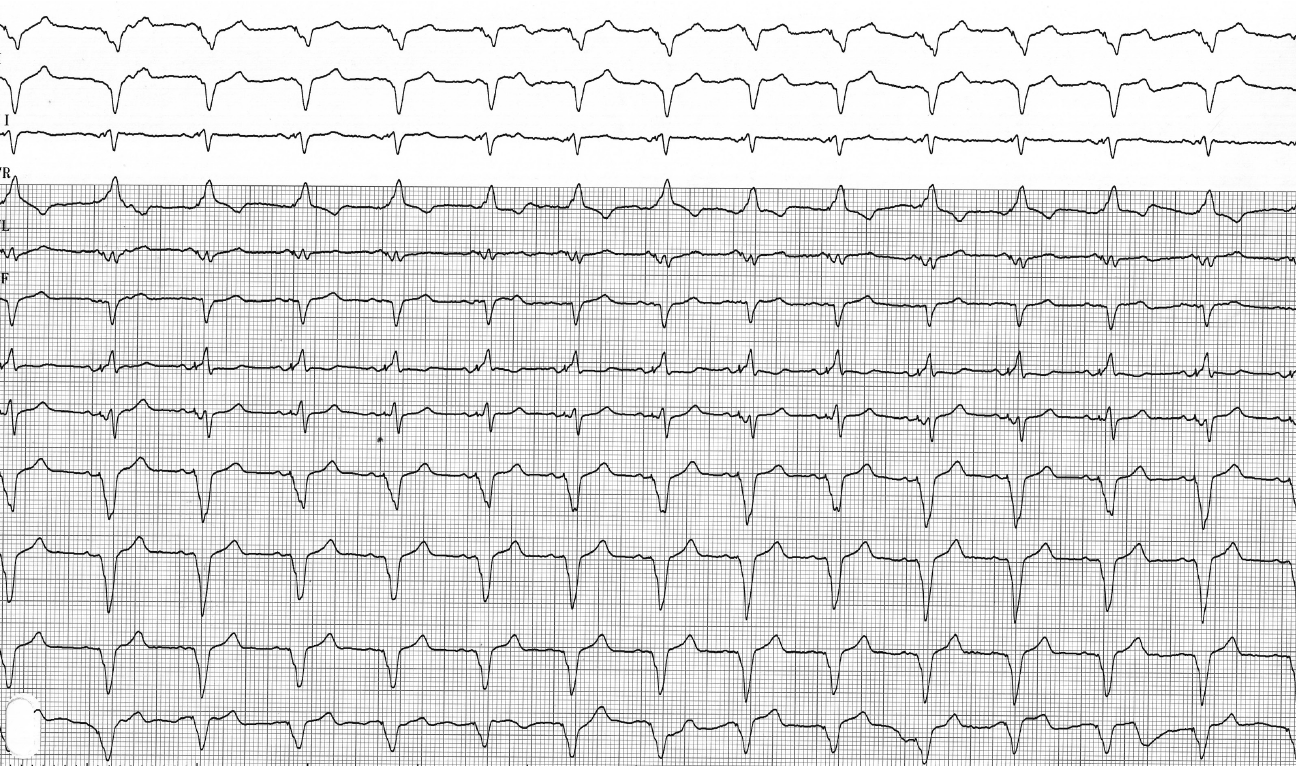
ECG recording taken after programming left ventricular pacing only; the QRS complex is much wider than during biventricular pacing, with marked negativity in DI and positivity in V1, consistent with the lateral position of the lead;
Commentary
The electrocardiogram is an essential tool in the follow-up of patients undergoing cardiac resynchronization therapy; it can raise suspicion of displacement leading to a loss of left ventricular capture, even though a definitive diagnosis is made through pacemaker interrogation and a chest X-ray. To facilitate follow-up by the referring cardiologist, it is helpful to have a baseline electrocardiogram for the patient showing spontaneous rhythm, right ventricular capture alone, left ventricular capture alone, and biventricular pacing. This makes it easy to identify loss of capture through comparison. Despite potentially significant remodeling in terms of ventricular volume, the appearance in each configuration changes relatively little over time, both in terms of QRS width and morphology.
To attempt to diagnose a loss of capture on the electrocardiogram, certain factors must be understood. The biventricular pacing pattern depends on the fusion of two different activation fields originating from the right ventricular lead and the left ventricular lead. The pattern observed during biventricular pacing varies among patients depending on the position of the two leads, the amount of myocardium depolarized by the right and left leads, respectively, the patients’ electrical and anatomical characteristics, and the degree of fusion with spontaneous activation.
The most common and clinically significant condition to diagnose is loss of left ventricular capture. The QRS duration is generally shorter during biventricular capture compared to right or left monoventricular pacing, but this criterion alone is not sufficiently discriminatory to demonstrate loss of capture. Diagnosis is easier when the right ventricular lead is located at the apex. In fact, apical right ventricular pacing is associated in the majority of cases with a positive QRS in DI and a negative QRS in the inferior leads. The axis is usually deviated to the left, and the QRS is almost never positive in V1. A negative QRS in DI and/or a positive QRS in V1 should be looked for.
In fact, the presence of either of these two findings (a negative wave in DI and/or a positive wave in V1) confirms the presence of effective left ventricular capture. A pattern consistent with right monoventricular pacing, however, does not rule out the existence of effective left ventricular capture but may be related to the predominant influence of the right lead on the QRS complex. The QRS duration is often shorter during biventricular pacing compared to the pattern seen with right-ventricular pacing. When the right ventricular lead is located in the upper septum or at the level of the infundibulum, diagnosing loss of left ventricular capture is much more difficult because the pattern in V1 and DI is no longer as consistent.
Right ventricular loss of capture is less common but less hemodynamically detrimental. The QRS complex during left ventricular pacing is often markedly widened. The QRS axis is upright or hyper-upright. Its morphology depends on the position of the left ventricular lead. The more lateral the lead, the more negative the QRS becomes in DI, with a right bundle branch block appearance. The more apical the lead, the more negative the QRS becomes in the inferior leads.

Trace description
Trace recorded after programming right ventricular pacing alone; the QRS complex is wider than during biventricular pacing, with marked negativity in the inferior leads consistent with the apical position of the lead;