

Boston Scientific - Implantation
Content
Introduction
After the implantation of first generation defibrillators, the procedure ended nearly systematically by the induction of VF to confirm the reliable detection and termination of the arrhythmia by the device and verify the integrity of the high voltage system. Failure to defibrillate, nowadays, is rare, a majority of patients undergo device implants for primary prevention, and ATP can terminate a large proportion of rapid VT. Furthermore, the maximum strength of the shocks delivered by the latest implantable defibrillators is higher and associated with a wider safety margin. This has prompted many implanting centres to reconsider the need for a systematic test at the end of the procedure and, instead, to proceed on a case-by-case basis.
The induction of VF enables the testing of the proper function of the implanted device and the verification of:
- the integrity of the high voltage system
- the reliable sensing and repeat sensing of the endocardial signals during VF
- a wide enough defibrillation safety margin.
Induction of ventricular fibrillation
Four different means are available to induce VF in Boston Science devices: shock‑on‑T, HF Burst and VFib induction.
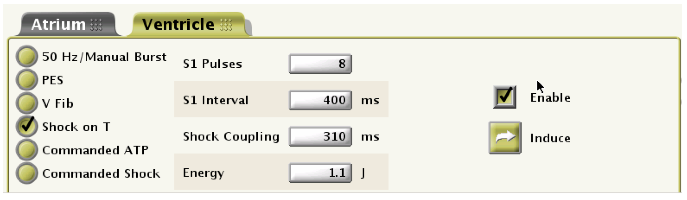
1. Shock‑on‑T : A ventricular arrhythmia (most often VF) is unduced by the delivery of a low energy shock during the ventricular vulnerable period. In practice, a ventricular stimulation sequence (nominally 8 stimuli), at a fixed rate (nominally 150 bpm or a cycle length of 400 ms) is followed by the delivery across the electrodes, of a low-energy electrical shock (nominally 1.1 J) during the ventricular vulnerable period (at a nominal coupling interval of 310 ms).
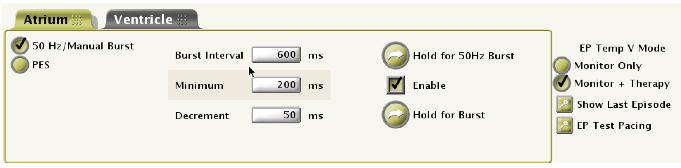
2. HF burst : a manual salvo of rapid pulses at a 20-ms (50 Hz) cycle length is delivered for as long as the operator presses on the switch and telemetry communication is maintained, up to 30 seconds.
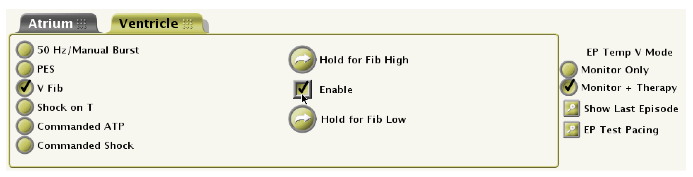
3. VFib induction : pacing the right ventricle across the high voltage electrodes at a very high rate and high amplitude, though the pulse strength is programmable from a weak waveform of 9 V/1.1 ms at 50 ms cycle length (20 Hz) to a strong waveform of 15 V/1.1 ms at 50 ms cycle length. The pulse train is delivered as long as the operator presses on the switch and the telemetry communication is maintained (up to 15 sec). This type of induction often causes a strong and painful stimulation of the adjacent muscle mass, requiring sedation or general anaesthesia.
4. induction by programmed electrical stimulation (PES): the aim is to induce an arrhythmia (most often VT) by programmed ventricular stimulation, i.e. a train of nominally 8 ventricular stimuli at a fixed rate (nominally at a 600-ms cycle length), followed by 1 to 4 premature stimuli.