Acceleration of VT by burst of ATP
Tracing
Manufacturer Abbott
Device ICD
Field Therapy
N° 38
Patient
This 35-year-old man presenting with arrhythmogenic right ventricular dysplasia underwent implantation of an Atlas single chamber ICD for VT complicated by syncope during beta-adrenergic blockade. He was seen after an episode of syncope and electrical shock during exercise.
Main programmed parameters
- VF zone at 222 bpm, VT zone at 179 bpm
- 8 cycles in the VF zone, 12 cycles in the VT zone
- Maximum sensitivity programmed at 0.5 mV
- VF zone: six 36-J shocks (maximum amplitude); VT zone: 3 bursts followed by single 10-J shock, followed by 3 shocks of maximum strength
- Effective discrimination in the VT zone
- VVI mode pacing at 40 bpm; VVI post-shock pacing mode at 70 bpm
Graph and trace
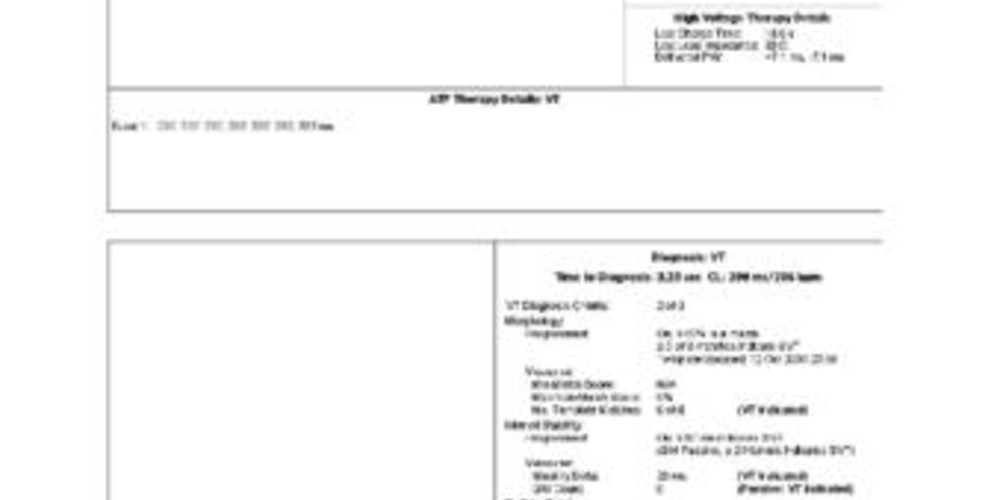
Episode of VT; the 3 discrimination criteria favour VT; the first delivered therapy is a burst of 8 stimuli with acceleration to the VF zone and delivery of a 36-J shock.
Tracing
- End of a previous episode;
- Sinus tachycardia;
- Probable VT (sudden onset, regular tachycardia, different morphology); the initial cycles are unclassified;
- VVI episode pacing mode after 4 T classified cycles;
- Diagnosis of VT after 12 cycles in the VT zone;
- Burst of 8 stimuli;
- Acceleration of the VT and redetection in the VF zone (after 6 F classified cycles); charge of the capacitors;
- Shock delivered at the end of charge, which lasted 18 sec;
- Successful shock and diagnosis of return to sinus rhythm.
Other articles that may be of interest to you




In this patient, the first sequence of ATP accelerated the arrhythmia to ventricular flutter detected in the VF zone. In some patients, the various sequences of ATP are arrhythmogenic, and transform systematically a hemodynamically stable, monomorphic VT into a fast, life-threatening VT or into VF. In a first step, one can lower the aggressiveness of the pacing sequences. Various settings can be programmed to vary the intensity of the sequences of ATP: 1) bursts are more aggressive than ramps, 2) when the pacing rate is a percentage of the tachycardia cycle, the lower the percentage, the stronger the sequence, 3) the greater the number of pacing cycles the more aggressive is the salvo, especially with a ramp, where the length of each consecutive cycle decreases, 4) the shorter is the shortest pacing interval reached by the ICD, the more aggressive is the sequence of ATP.
The salvo of ATP delivered in this patient (burst of 8 cycles at 232 ms) was not particularly aggressive. When ATP is systematically arrhythmogenic or unsuccessful (the bursts do not terminate or accelerate the tachycardia), it may be recommended to not program these therapies and to program a 5-10 J shock as first therapy instead. In this patient presenting with arrhythmogenic right ventricular dysplasia the arrhythmia was exercise-induced. A release of catecholamines was probably the cause of the initial arrhythmia and might have contributed to the arrhythmogenic properties of the salvo of ATP. A closely followed administration of a beta-adrenergic blocker seems in order.