PR Logic and sinus tachycardia
Tracing
Manufacturer Medtronic
Device ICD
Field Discrimination
N° 34
Patient
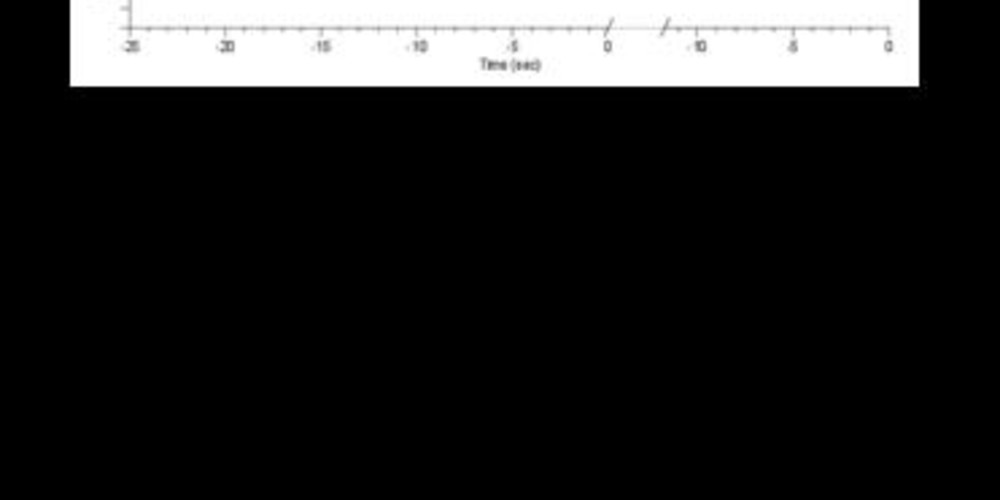
Patient with ischemic cardiomyopathy implanted with a dual-chamber ICD (Evera XT DR) with slow VT episodes (125 beats/minute); programming of a slow VT zone at 520 ms; this tracing highlights the functioning of the PR Logic algorithm and the diagnosis of sinus tachycardia.
Graph and trace
The graph shows a 1:1 tachycardia with a gradual slowing of the rate; no therapy was delivered following the diagnosis of sinus tachycardia.
- the EGM shows a 1: 1 tachycardia;
- diagnosis of sinus tachycardia;
- the Sinus Tach option was programmed to ON.
Other articles that may be of interest to you



This patient had multiple episodes of symptomatic slow VT requiring special programming with a relatively low VT zone (520 ms), increasing the risk of overlap with the sinus rates observed during exertion. This episode presents the characteristics of a sinus tachycardia (1: 1 ratio between the atria and ventricles, progressive acceleration and deceleration) well diagnosed by PR Logic.
When the Tach sinus option is programmed to ON, various steps are used for arriving at the diagnosis of sinus tachycardia: