2/1 block during exercise
Tracing
Manufacturer Medtronic
Device PM
Field Programming for exercise
N° 27
Patient
A 28-year-old woman surgically implanted with a triple-chamber pacemaker (1 atrial lead, 2 left ventricular leads) for congenital complete atrioventricular block; programming in DDD mode (single left ventricular lead) 60-120 beats/minute; sensation of blockpnea on exertion; exercise test (bending of the legs) with the telemetry head positioned over the pulse generator; EGM tracing recorded during vigorous effort with, from one beat to the next, sensation of blockpnea (exercise was halted at this precise moment to obtain a high quality tracing).

Graph and trace
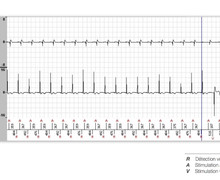
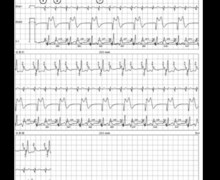
Tracing 27a: vigorous exertion;
- AS-VP interval with programmed AV delay;
- P wave blocked since falling within the PVARP (AR);
- new AS-VP interval with programmed AV delay;
- new P wave blocked since falling within the PVARP (AR); 2/1 block;
- the sudden drop in rate favors the emergence of a junctional escape rhythm (narrow QRS); atrioventricular dissociation;
- repetition of 2/1 intervals alternating with junctional escape;
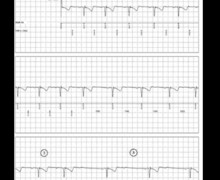
Tracing 27b: tracing recorded during recovery;
- 2/1 block with a followed P wave (AS) and a P wave in the blocked refractory period (AR);
- slowing of the heart rate during recovery and return of AS-VP intervals with 1/1 conduction.
Other articles that may be of interest to you

This tracing allows emphasizing certain programming specificities in young patients with preserved activity and contractile function implanted with a pacemaker:
This patient presents a congenital complete atrioventricular block without anterograde or retrograde conduction at rest or during exertion. The risk of PMT is therefore zero. This allows programming a PVARP as short as possible with an adjustable AV delay. The 2/1 point should be pushed beyond the maximum capacities of the patient.