Long PR and second MVP version
Tracing
Manufacturer Medtronic
Device PM
Field MVP
N° 11
Patient
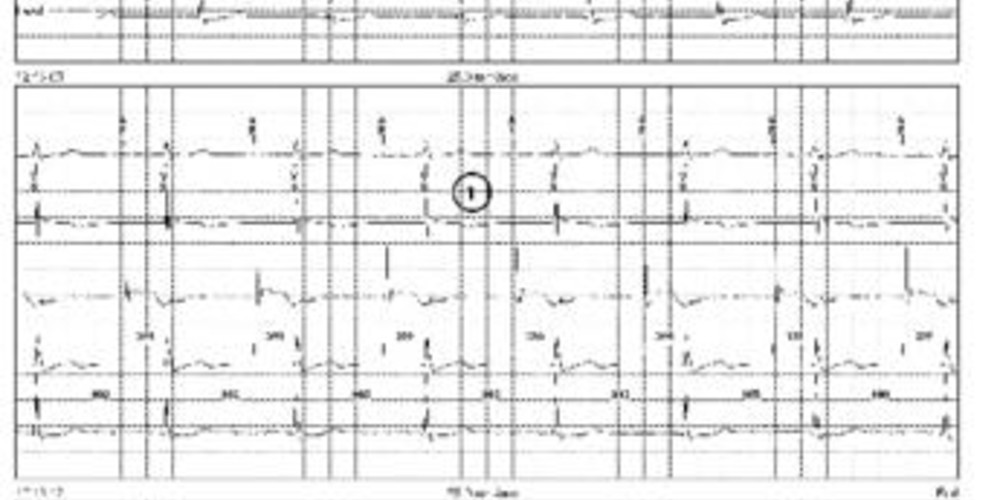
Same patient as in previous tracing.
Graph and trace
Programming of the MVP mode with switching due to long PR (programmed limit value 350 ms); progressive increase in the pacing rate and analysis of atrioventricular conduction;
- atrial pacing at a rate of 60 beats/minute with 1/1 conduction and AP-VS intervals between 315 and 325 ms;
- programming of a rate of 70 beats/minute;
- 1/1 conduction and AP-VS intervals between 330 and 337 ms;
- programming of a rate of 80 beats/minute;
- 1/1 conduction and AP-VS intervals between 342 and 350 ms; the average over 4 consecutive cycles of the AP-VS interval remains consistently under 350 ms, the programmed limit value;
- programming of a rate of 90 beats/minute;
- 1/1 conduction; the average of the 4 consecutive AP-VS intervals (347, 342, 362, 357 ms) is greater than 350 ms, the programmed limit value;
- switching to DDD mode with programmed AV delay;
- ventricular pacing for 1 minute (DDD mode);
- after one minute in DDD mode, analysis of atrioventricular conduction; on this cycle, presence of an AP-VS interval > 350 ms;
- resumption of the DDD mode.
Other articles that may be of interest to you




When the PR interval is extremely prolonged, the physiological activation/contraction sequence between atria and ventricles is no longer observed, leading to a contraction of the atria while the mitral valves are closed, which can be associated with the presence of symptoms. These tracings illustrate the new functionality of the MVP algorithm with the possibility of switching when the PR interval exceeds a programmable value. The device measures the PR interval (atrial sensing, AS-VS) or AR interval (atrial pacing, AP-VS) averaged over 4 consecutive cycles. If the average of the last four PR or AR (no difference in value whether the atrium is sensed or paced) exceeds this limit, the device switches to DDD(R) mode. The first atrioventricular conduction verification occurs 1 minute after switching to the DDD(R) mode. During this verification, if the PR or AR interval remains prolonged and greater than the programmed value, the device continues in DDD(R) mode. The interval between each conduction control is then doubled (2, 4, 8... minutes to a maximum of 16 hours). For this patient, we can see that the first version of the algorithm would not have led to a switching in DDD mode (absence of blocked P waves) and that at the time of conduction verification, it would have returned to ADI mode (long AR but 1/1 conduction).
By default, the long PR function of the MVP algorithm is programmed to OFF. It is probably necessary to reserve the programming of this feature for patients with symptoms on exertion. Indeed, a similar value of PR interval duration may be acceptable at rest but problematic on exertion. A value of 300 to 350 ms for the PR limit value probably corresponds to a good compromise for limiting the occurrence of symptoms on exertion while avoiding iterative commutations, even if an individual optimization of this parameter can be proposed.