Loss of biventricular pacing due to long PR interval and P-wave in the PVARP
Tracing
Manufacturer Medtronic
Device CRT
Field Standard parameters
N° 19
Patient
65-year-old man, implanted with a triple-chamber defibrillator Protecta XT CRT-D for primary cardiomyopathy with sinus dysfunction, left bundle branch block and long PR interval; routine follow-up 6 months after implantation; recording of spontaneous ventricular sensed event.
Graph and trace
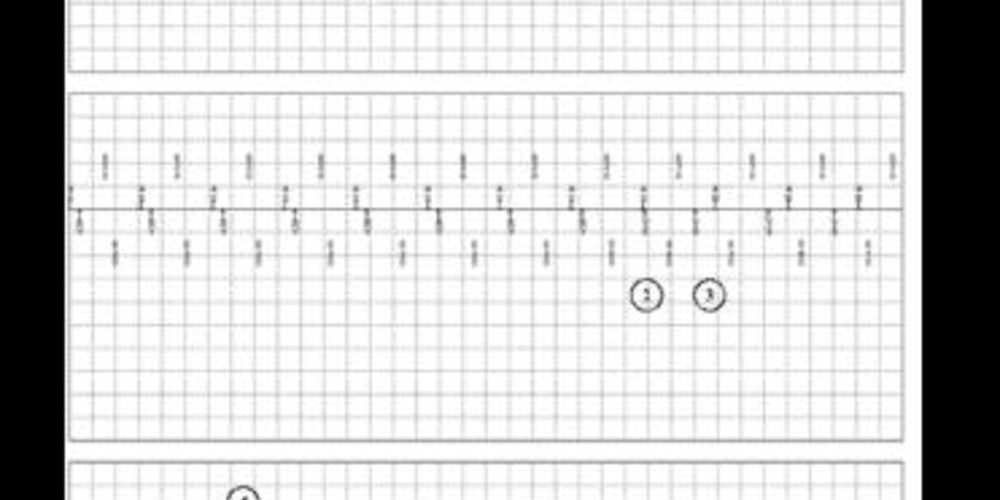
Episodes of ventricular sensed event in the device memory
- atrial sensing and biventricular pacing (AS-BV);
- probable ventricular premature beat;
- atrial activity falling in the PVARP, no AV delay and absence of biventricular pacing;
- consecutive AR-VS cycles with prolonged loss of biventricular pacing;
RV threshold test in VDI mode at 90 bpm - ventricular capture with dissociated atrial rhythm followed by conduction from the atrium to the ventricle: AS-VS cycles with long PR interval; interruption of the test;
- during the last pacing of the threshold test (VP), prolongation of the PVARP; sinus activity falling in the PVARP;
- successive AR-VS cycles with a long PR interval and sinus P wave in the PVARP;
- moderate sinus pause allowing the P wave to fall outside the PVARP;
- recovery of biventricular pacing;
Change in device programming (atrial tracking recovery algorithm is turned ON); the patient is discharged
New episodes of ventricular sensing recorded by the device - atrial sensing and biventricular pacing (AS-BV);
- ventricular quadruplet;
- atrial activity falling in the PVARP, no AV delay and absence of biventricular pacing; succession of AR-VS cycles with prolonged loss of biventricular pacing;
- intervention of the atrial tracking recovery algorithm; shortening of the PVARP; recovery of the biventricular pacing.
Other articles that may be of interest to you


This example illustrates a relatively common cause of loss of biventricular pacing in patients with long PR interval. Following a loss of atrioventricular synchrony (PVC, pacing threshold, etc.), a P-wave falls within the PVARP, and does not launch a new AV delay. As a result, spontaneous conducted ventricular events appear. The probability that the next P-wave falls within the PVARP and maintains the phenomenon increases with PR duration (the longer the duration, the greater the risk), the sinus rate (the faster the rate, the greater the risk) and the programming of certain algorithms (PVARP extension after PVC, auto-threshold procedure, automatic PVARP). The programming of these algorithms should be discussed case-by-case, particularly in CRT patients with long PR (higher risk of occurrence of this type of phenomenon with a theoretically lower risk of PMT in the presence of impaired AV conduction). Programming the atrial tracking recovery algorithm interrupts the repetition of these cycles. This algorithm must therefore be programmed to ON.