Syncope during complete atrioventricular block
Tracing
Manufacturer Medtronic
Device ILR
Field Reveal DX / Reveal XT
N° 4
Patient
An 81-year-old woman presented with 2 sudden episodes of syncope without trauma. The ECG reveals normal PR and QRS intervals at 190 and 95 ms, respectively. A 48-h ambulatory ECG was normal. Electrophysiological studies revealed no intra or infra-Hisian block. A Reveal DX was implanted.
Graph and trace
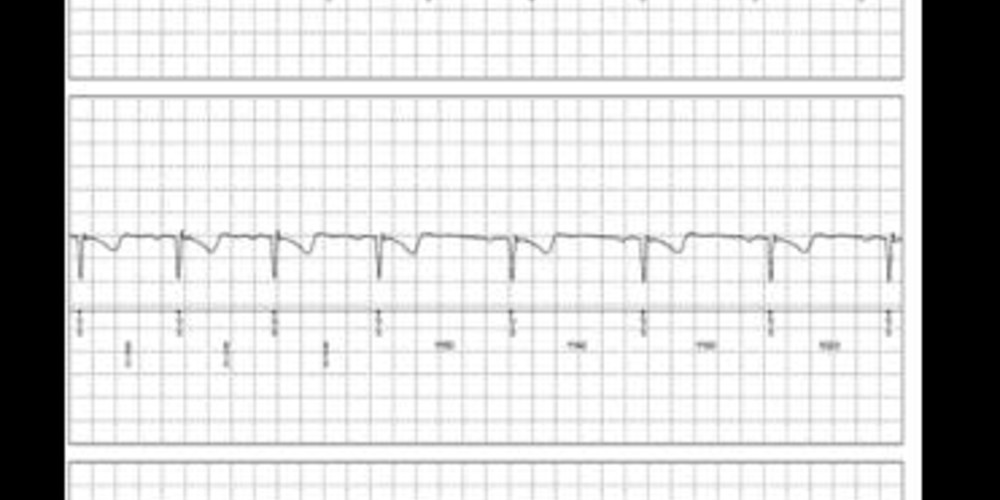
The patient suffered an episode of syncope with facial trauma. Since the patient was unable to record the episode, the following information was automatically collected by the device.
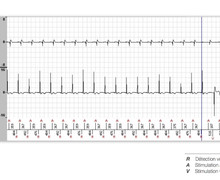
- normal sinus rhythm with 1:1 conduction, a normal PR interval and a narrow QRS;
- slight lengthening of the PR interval;
- development of 2:1 2nd degree atrioventricular block;
- several consecutive P-waves were blocked, with diagnosis of bradycardia (B);
- detection of an episode of asystole (AD).
Other articles that may be of interest to you



This clinical and electrocardiographic presentation likely corresponds to idiopathic paroxysmal atrioventricular block with
The ILR revealed a conduction disorder previously difficult to demonstrate. This patient underwent implantation of a pacemaker, which prevented further recurrences. Permanent pacing has been uniformly effective in similar cases published in the medical literature. This clinical case highlights the advantages and limitations of this type of device. On the one hand, a diagnosis was made after recurrence of syncope complicated by facial trauma. On the other, it seemed unacceptable to proceed with a pacemaker implant as a first step in this patient, whose ECG was normal and electrophysiological studies were non-contributory.
The activation of the ILR after the onset of an episode, using the Patient Assistant, may be impossible by patients who have