Detection of ventricular fibrillation and successful treatment by a shock
Tracing
Manufacturer Medtronic
Device ICD
Field Therapy
N° 11
Patient
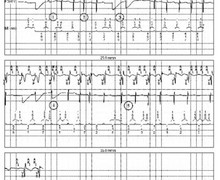
Patient implanted with a single-chamber ICD (Protecta VR) for ischemic cardiomyopathy and hospitalized for several syncopal episodes with electrical shocks; this tracing shows a control episode of the "normal" functioning of an ICD with correct detection of ventricular fibrillation and successful treatment by a maximum electrical shock

Graph and trace
The graph initially shows a steady regular rhythm, followed by a sudden acceleration in the VF zone, the detection of a VF episode and finally a maximum electrical shock resulting in a slowing of the ventricular rate.
- the EGM shows an extremely rapid and polymorphic ventricular arrhythmia corresponding to a VF episode correctly detected by the device;
- after 30 intervals classified as FS (programmed initial detection 30/40), initial detection of a VF episode;
- the charging of the capacitors begins only in the presence of VS markers;
- when charging is complete, confirmation phase followed by delivery of electrical shock (35 Joules); clear slowing of the ventricular rate
Other articles that may be of interest to you
EGM recordings


Implantable defibrillators have been historically developed to prevent the risk of sudden death and reduce malignant ventricular arrhythmia by electrical shock. In the VF zone, a maximum of 6 shocks can be delivered for a single episode. While the amplitude of each of the shocks can be programmed independently, it is customary to program an amplitude at maximum capacity of the device (35 Joules) for shocks 2 to 6. In contrast, the amplitude of the first shock can either be programmed to the maximum capacity of the device, or to a value lowered by 10 Joules (25 Joules), or to a lower amplitude tested during an induction procedure. Programming a first shock of average amplitude (between 15 and 20 Joules) allows shortening the charging time and the delay between the onset of the arrhythmia and the delivery of the electrical shock and, in certain specific cases, can reduce the risk of loss of consciousness (an important problem for drivers, for example). The choice of the amplitude of the first shock in the VF zone therefore represents a compromise: an average energy may suffice to terminate the VF after a short charging time, however if unsuccessful, the second maximum energy shock will be delivered after a long total VF time; an immediate high energy will be more efficient on the VF, but at the cost of a longer initial charging time.
The shock waveform is not programmable on MedtronicTM devices, the electrical shocks delivered are necessarily biphasic without possible modification; indeed, while the first available devices delivered monophasic shocks, the introduction of biphasic shocks on the more modern platforms have enabled to significantly reduce the defibrillation thresholds and the risk of re-induction. The direction of the shock waveform is reversed with a non-modifiable 50/50 tilt. The polarity can be programmed independently for the 6 shocks of the series with 2 possible options: B>AX and AX>B; B corresponds to the right ventricular coil and AX to the active can and superior vena cava coil; in anodic shock (B>AX), the right ventricular coil constitutes the anode for the first phase and the cathode for the second; conversely, in cathodic shock (AX>B), the right ventricular coil constitutes the cathode for the first phase and the anode for the second phase. The shock vector can be modified when the implanted lead is double-coiled; when the lead is single-coiled, the only available vector is that between the right ventricular coil and the active can; when the lead is double-coiled, 3 options are programmable: single-coil (right ventricular coil – active can), double-coil (right ventricular coil – active can + upper vena cava coil), cold can (right ventricular coil - upper vena cava coil).