Erroneous single chamber discrimination: atrial fibrillation
Tracing
Manufacturer Abbott
Device ICD
Field Discrimination
N° 42
Patient
This 71-year-old recipient of a St Jude medical Analyst Accel single chamber ICD implanted for primary prevention in the context of ischemic cardiomyopathy suffered from episodes of paroxysmal AF and was seen on routine follow-up.
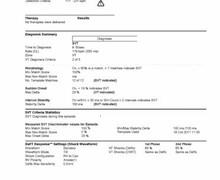
Main programmed parameters
- VF zone at 222 bpm, VT zone at 171 bpm
- 12 cycles in the VF zone and 20 cycles in the VT zone are needed for the diagnosis
- Effective discrimination programmed in the VT zone
- VT diagnosis criterion: 2 out of 3
- Morphology: ON (60% 5 of 8)
- Stability: ON 45 ms; detection window: 12 intervals
- SIH: 2 intervals
- Sudden onset: ON, 18%

Graph and trace
Tracing
- irregular, relatively slow ventricular rhythm (probable AF);
- initial cycle classified in the tachycardia or fibrillation zone of the episode (marked F on this tracing). The gradual versus sudden onset of the tachyarrhythmia is ascertained from this pivotal cycle onward; furthermore, the count of cycles classified as sinus versus non-sinus that are added to the SIH counter starts from this cycle;
- from this complex on, 12 cycles are analyzed, during which stability is ascertained;
- from this complex on, 8 cycles are analyzed, during which morphology is examined;
- diagnosis made by the device when the VT counter is full (12 cycles classified as T); the 8 ventricular electrograms analyzed for the morphology criterion were ruled similar (ν), as the percentage of resemblance remained consistently above the programmed 60% threshold. The sudden onset criterion favored VT. Out of 12 analyzed cycles, the second shortest and the second longest, respectively measured 297 and 320 ms, representing a 23 ms delta (rounded up to 25 ms), a criterion in favor of VT. However, starting with the first F cycle, 2 VS and 3 non-classified intervals brought the SIH counter to 5 à diagnosis of SVT à no therapy delivered;
- redetection after 6 cycles classified T: the sudden onset criterion, which was initially fulfilled, was not re-analyzed (this criterion is re-analyzed when initially negative). While morphology remained in favor of SVT, the SIH counter (which measures 6 redetection complexes and 6 complexes preceding the diagnosis of SVT) was now in favor of VT in absence of VS or unclassified intervals. Since 2 out of 3 criteria were in favor of VT à diagnosis of VT;
- burst of 8 complexes;
- persistence of AF; however, return to sinus rhythm was diagnosed (3 consecutive VS or VP without intervening T or F cycles).
Other articles that may be of interest to you


EGM recordings

This tracing highlights the limitations of programming 2 out of 3 VT diagnosis criteria in the discrimination of episodes of AF with a rapid ventricular rate. The initially irregular rhythm and similar morphology were accurately recognized. The rhythm later stabilized and 2 criteria out of 3 indicated VT, prompting the delivery of inappropriate therapy despite the accurate identification of SVT by the morphology criterion. This patient would probably have benefited from increasing the device specificity and the programming of discrimination by 3 out of 3 criteria, in which case all criteria needed to be fulfilled for a diagnosis of VT. A discrimination solely based on morphology may also be appropriate in this patient.