Optimization of the AV delay in a patient with complete AV block
Tracing
Manufacturer Medtronic
Device CRT
Field AV & VV delays optimization
N° 8
Patient
74-year-old man implanted with a triple chamber pacemaker Consulta CRT-P for idiopathic dilated cardiomyopathy with complete AV block; pacemaker interrogation 3 days post implant.
Graph and trace
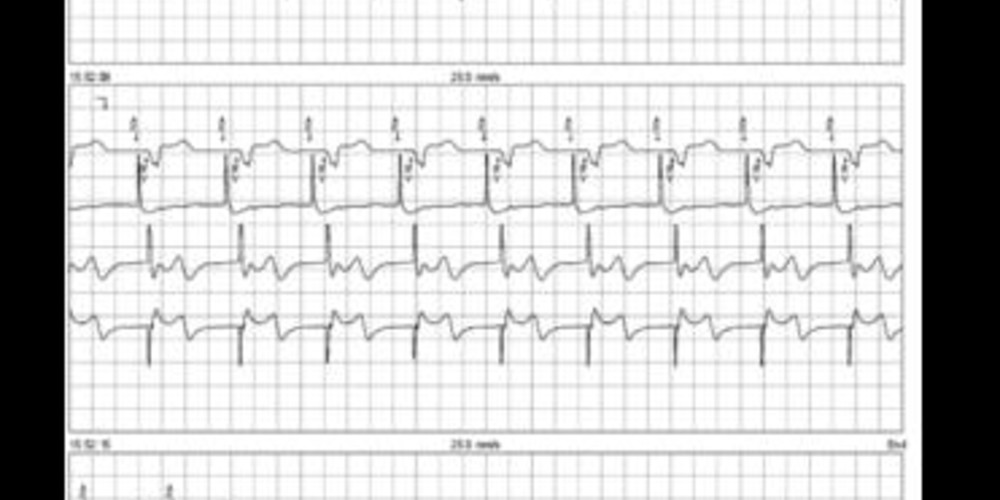
The first line corresponds to an electrocardiographic lead with superimposed markers (MA), the second line to the bipolar atrial recording (EGM1), the third line to the bipolar right ventricular EGM (EGM3) and the fourth line to the distal (tip) LV / RV coil lead (EGM2)
- the programmed paced AV delay is short (100ms); atrial paced rhythm and biventricular pacing (AP-BV cycles); on the atrial EGM, we see that the ventricular depolarization occurs just in the middle of the atrial depolarization;
- identical AV delay;
- extension of the paced AV delay to 180 ms;
- the appearance of the ventricular EGM is not impacted by the change in programming; the ventricular depolarization now occurs at the end of atrial depolarization.
Other articles that may be of interest to you




Atrial contraction contributes to 20-30% of cardiac output at rest in heart failure patients with systolic dysfunction, this contribution increasing with exercise. Heart failure patients with left bundle branch block often display atrioventricular dyssynchrony with a shortened filling time, a merging of the E wave and A wave, and diastolic mitral regurgitation. In CRT patients, the programming of a short AV delay allows anticipation of the E wave, dissociation of the E and A waves and a prolongation of the filling time. The AV delay should not be programmed too short since it causes amputation of the A wave by mitral closure.
AV optimization is recommended after implantation of a triple-chamber pacemaker or defibrillator even if the level of clinical evidence is modest. Indeed, there are large interindividual variations in intra-atrial and intra-ventricular conduction disorders, leading to marked differences in optimal AV delay, theoretically justifying a tailored adjustment for each patient. The sensed and paced AV delays are independently programmable and therefore must also be optimized independently.
In patients with a high-grade atrioventricular block or with a very prolonged PR interval, variations in AV delay have no direct effect on the degree of ventricular capture or fusion. The pattern of the paced QRS remains identical since there is no merging with any potential spontaneous QRS. During optimization of the AV delay, it is possible to concentrate on only the parameter selected for the optimization: the longest filling time without amputation of the A wave, reduction of mitral regurgitation, search for the maximum cardiac output, etc. Ideally, the optimal AV delay corresponds to the setting that allows the best compromise between all of these parameters.
In this patient, ultrasound revealed a clear amputation of the A wave by mitral closure for the first paced AV delay (100 ms). Mitral filling appeared to be better adapted for the second (180 ms) with a longer filling time with dissociation of the A wave and the E wave and non-amputated A wave. The qualitative pattern of the mitral filling appeared reproducible. In contrast, a large cycle-to-cycle variation of the signals made the analysis of the sub-aortic TVI poorly reproducible and thus poorly interpretable.