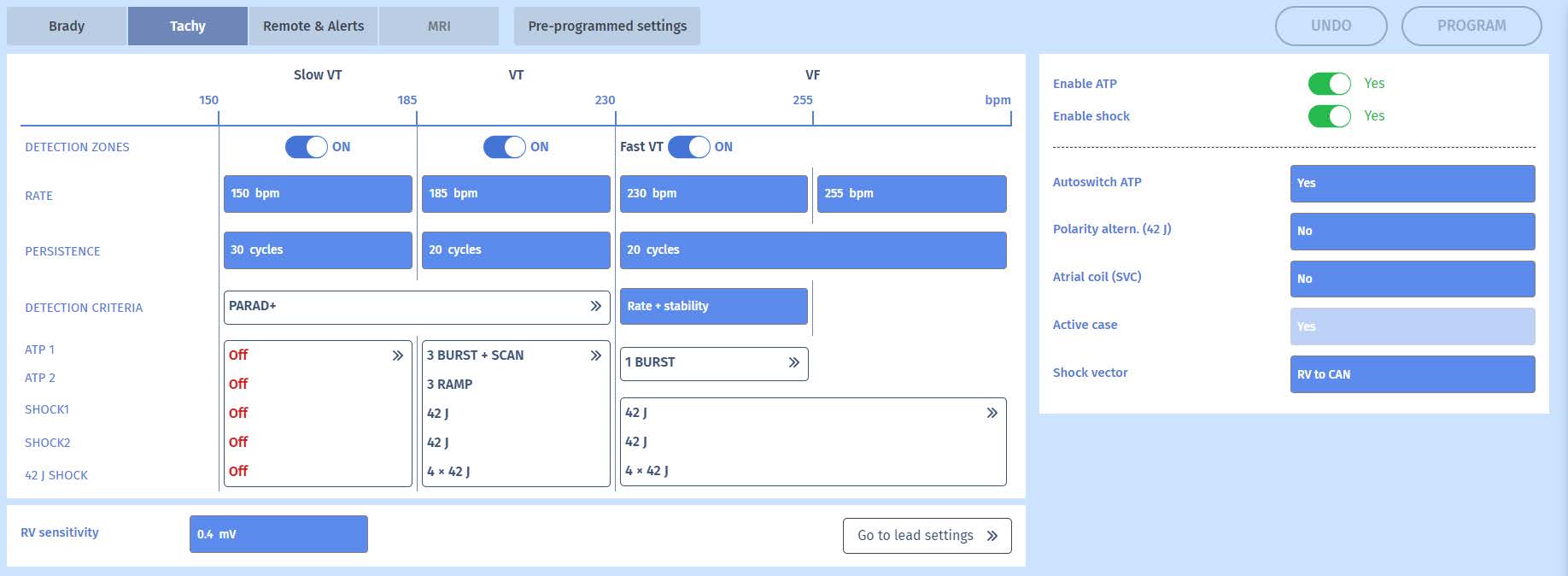
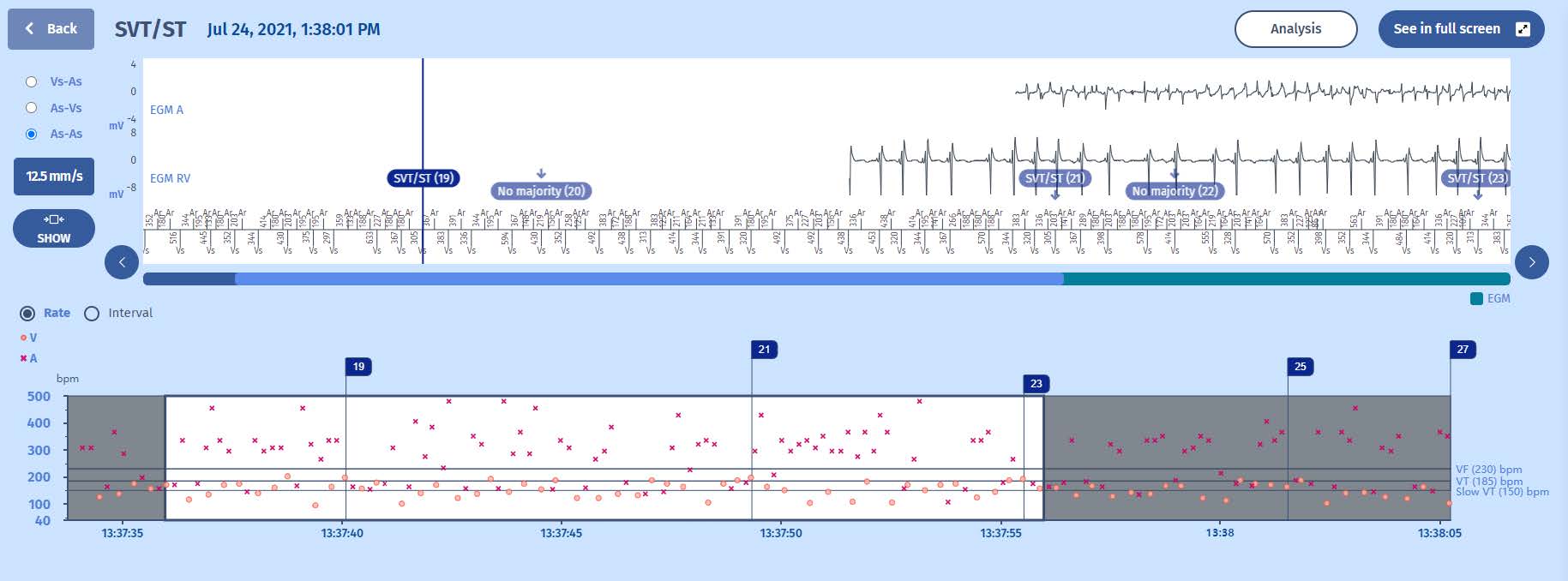
On the bottom of the two figures we can appreciate the gradual onset of the tachycardia and the gliding into the VT zone. This is most typical for sinus tachycardia. After various markers, we see the therapies being delivered: bursts, ramps and shocks.
EGM
This is a long episode so only snippets of EGM are made available but it shows the same features as seen in the interval plot; the appearance of gradually faster ventricular events. As it is a single-chamber ICD with only a ventricular lead, we do not see an atrial channel. Where we would normally see an atrial channel, we now see a far field channel between the can and the RV coil, which is similar to a surface ECG. On this channel we can appreciate more of the QRS morphology and compare it to other episodes or live EGM which in this case is identical. This confirms the diagnosis of inappropriate therapies for sinustachycardia misdiagnosed as VT. While competitors use this information as a criterion for discimination (with varying results), it is not the case for
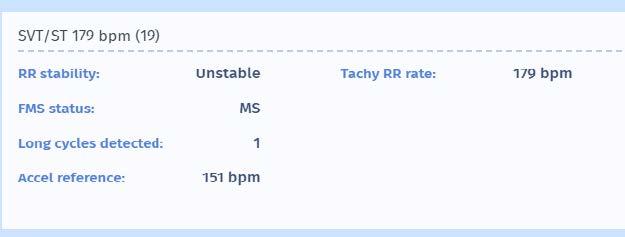
MicroPort devices, which rely on atrial leads for discrimination, and in absence of atrial leads, rely on sudden onset and stability criteria. In this case we can see that while initial diagnosis markers of SVT appear, the long intervals (post compensatory pauses after premature ventricular complexes) make the ICD believe that there is a sudden onset of VT (which is not the case). As the tachycardia is within the VT zone (>170/min), stable and considered as sudden onset, it is diagnosed as VT. As these three features do not change during the persistence, the therapies will keep being delivered until the ventricular rate slows down out of the VT zone. This is problematic as the sinus tachycardia tends to accelerate when a patient suffers from shocks.