- the defibrillation threshold does not correspond to a fixed value; several shocks at maximum energy are ineffective in this patient, whereas the fourth shock of the same amplitude averts a dangerous scenario
- a shock is effective if a sufficient critical mass of myocardium is depolarized, establishing an intramyocardial voltage gradient; an electric shock is ineffective if a residual mass of fibrillating myocardium remains, or if there is immediate reinduction in areas where the induced gradient is insufficient; these tracings show that the shock terminates a disorganized ventricular arrhythmia with almost immediate reinitiation
- when the first shock is ineffective, a vicious cycle sets in; prolonged duration of VF worsens hemodynamics, ischemia and myocardial stretch, reducing the probability of a successful subsequent shock
- a shock most often terminates episodes of ventricular arrhythmia and is the basic treatment of the defibrillator; however, the shock can sometimes be pro-arrhythmogenic and, as in this patient, transform an organized VT into a potentially lethal VF (stable VT before the first shock and VF afterwards)
- the effect of a shock varies according to the energy delivered; for low energy, a shock in a vulnerable period can induce arrhythmia; the upper limit of vulnerability corresponds to the lowest energy, applied in a vulnerable ventricular period, which does not induce ventricular fibrillation; this value is correlated with the defibrillation threshold; the probability of termination then increases following an exponential probability curve as a function of the amplitude of the shock delivered (synchronized to the R wave); above a certain value, the risk of re-inducing an arrhythmia also increases, limiting the chances of successful therapy; a shock with too high an amplitude can damage myocardial tissue
- in this patient, the first shock degraded a monomorphic, organized arrhythmia into a polymorphic, chaotic one, suggesting the existence of a high defibrillation threshold; the shock failed to capture a sufficient quantity of ventricular myocardium, and instead created sufficient pro-arrhythmogenic myocardial heterogeneity to generate multiple reentry circuits; it is therefore not surprising that subsequent delivery of the same amount of energy did not terminate the episode of VF induced by the first shock, and that several shocks were required (immediate reentry); to defibrillate, a shock must significantly modify the trans-membrane potential to interrupt the waves of fibrillation; however, if new fronts are created, immediate reentry of VF may be observed
- in this patient, safety seemed compromised with few reprogramming options available; a coil positioned in the coronary sinus was added; in fact, a shock delivered between two electrodes in contact with or in the immediate vicinity of the cardiac mass is more likely to be effective by extending the induced electric field over a larger volume
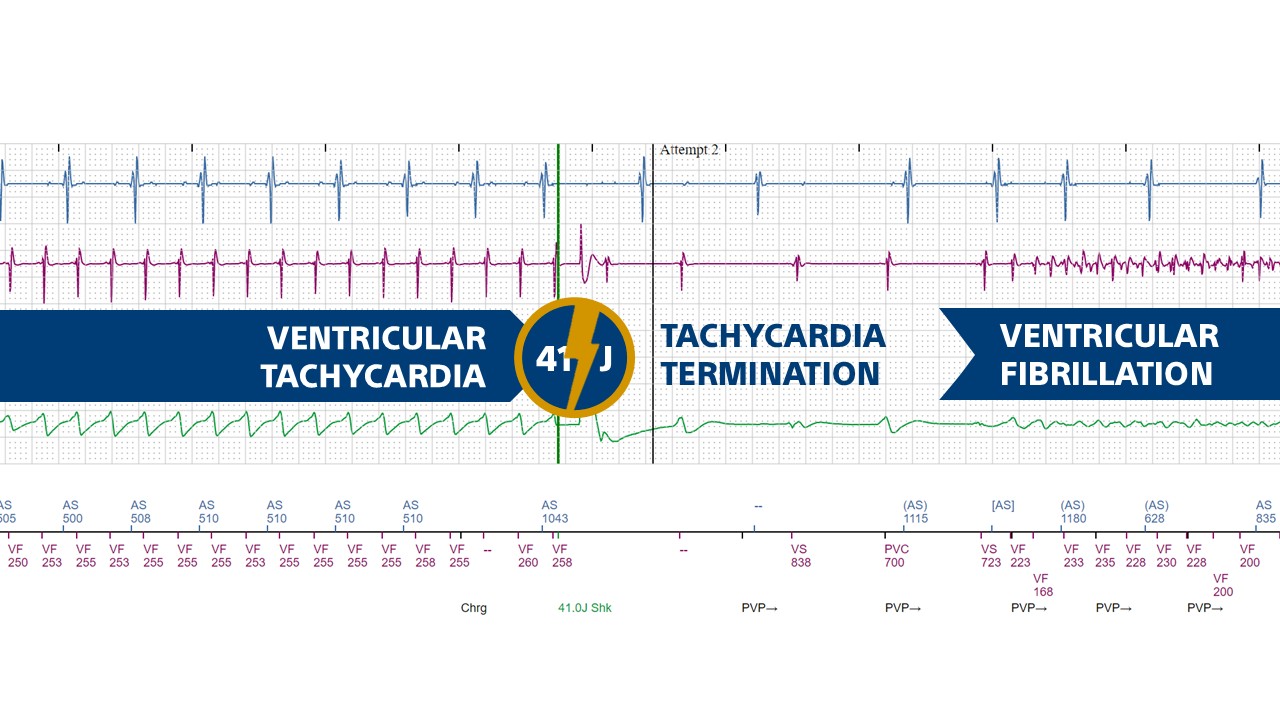
The tracing shows how the shock delivered during a monomorphic tachycardia (VT) interrupts the tachycardia with immediate reinduction of a polymorphic, disorganized, low-voltage arrhythmia (VF).

