- children implanted with a defibrillator are very much a minority compared to adults (less than 1% of defibrillator wearers are children)
- the indications for defibrillation in pediatrics have not been the subject of randomized studies and are based on expert consensus; although initially reserved for secondary prevention indications, the percentage of implantations in primary prevention has now increased considerably
- there are no devices or leads specific to this age group that have been adapted to children’s anatomical characteristics
- the risk of inappropriate therapies is increased in children due to a higher risk of lead fracture as children grow and subject leads to greater stress; higher baseline heart rates and frequent episodes of sinus tachycardia, supraventricular tachycardia or T-wave oversensing also contribute
- there is no standardized programming and the various parameters having to be adjusted and optimized on a case-by-case basis; in secondary prevention of resuscitated sudden cardiac death, a single VF zone is usually programmed with a relatively high minimum rate, higher than the heart rate range corresponding to sinus tachycardia; to reduce the risk of inappropriate therapies, it’s customary to program relatively long initial durations, as arrhythmia is generally well tolerated in children, even for high ventricular rates, and syncope is usually relatively delayed
- the programming in this young patient may seem surprising, with an initial duration in the VF zone of 1 second; this patient initially presented with traumatic syncope and to avoid future falls, a decision was made to deliver the shock before loss of consciousness; the interval between the onset of arrhythmia and the shock was around 6 seconds (approx. 2 seconds for the 8 initial cycles, initial duration of 1 second, charge time of 2.7 seconds, diversion window of 500 ms)
- in children, the amplitude of the first shock is generally programmed to be relatively low (sometimes 2 to 5 Joules in neonates); an amplitude of 1 Joule/kg provides high efficacy with limited deleterious effect
- telemonitoring is essential to reduce inappropriate therapies in children (as in adults …).
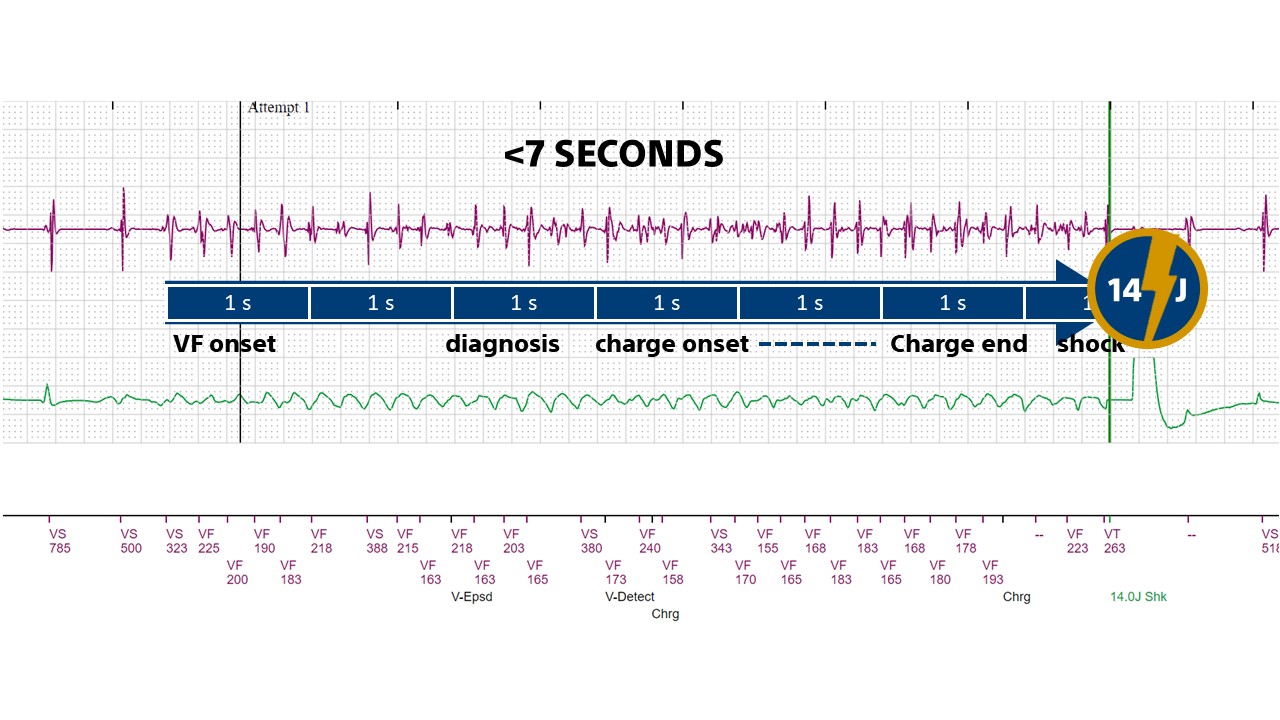
This figure shows the time interval in this young patient between the onset of arrhythmia and the moment when the shock is delivered; this interval is broken down into 8/10 criteria, initial duration in the VF zone, capacitor charging, confirmation at the end of charging, etc.

