- implantable defibrillators were historically developed to prevent the risk of sudden death and terminate malignant ventricular arrhythmia via a shock
- this tracing illustrates normal defibrillator operation during a VF episode: correct arrhythmia detection, capacitor charging, confirmation at the end of charge and effective shock
- the arrhythmia is immediately extremely rapid, polymorphic and disorganized, consistent with VF; any attempt to terminate this type of arrhythmia by anti-tachycardia pacing is doomed to fail, and a shock remains the standard therapy in this setting
- detection is correct and there is no discrimination of arrhythmia origin in this ventricular rate range
- for a Boston Scientific defibrillator, a series of 8 shocks can be programmed in the VF zone
- the amplitude of shocks 3 to 8 is not programmable and is always the maximum (41 Joules)
- the amplitude of the first 2 shocks is programmable, even though the amplitude of the second shock must be at least equal to that of the first; the amplitude of the second shock is generally programmed at the device’s maximum capacity
- the amplitude of the first shock can either be programmed to the maximum capacity of the device, or to a lower value of 10 to 20 Joules; programming a first shock of intermediate amplitude makes it possible to reduce the charge time and the delay between arrhythmia onset and shock delivery, and may in certain specific cases reduce the risk of loss of consciousness; the choice of the amplitude of the first shock in the VF zone therefore represents a compromise: medium energy may be enough to terminate VF after a short charge time, but if this fails, the second, maximum-energy shock is delivered after a long total duration in VF; maximum energy is more effective from the outset, but at the cost of a longer initial charge time
- international recommendations state that it is reasonable (class IIA recommendation) to program the maximum amplitude in VF zones from the outset, unless an induction test has shown efficacy at a lower amplitude.
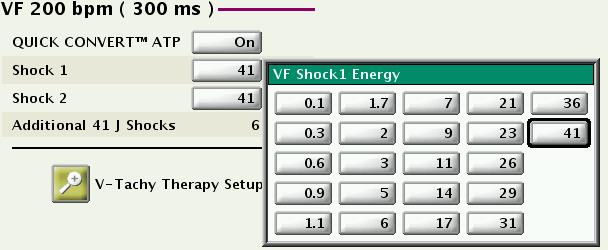
This figure shows the various programming options for the amplitude of the first shock in the VF zone; the amplitude of the second shock is also programmable but must be at least equal to that of the first; the amplitude of shocks 3-8 is necessarily maximum (41 joules; in the VF zone, 8 shocks can be delivered).

