40-year-old man implanted with an Incepta single-chamber defibrillator for spontaneous type 1 Brugada syndrome with a syncopal episode
ventricular lead positioned at the septum with average sensing of 3.5 mV in sinus rhythm
induction of VF at the end of the implantation procedure with ventricular sensitivity at 1 mV
Summary
episode of induced VF
charge diverted due to reconfirmation failure (abandoned attempt)
the arrhythmia is redetected and a 21 Joule shock is delivered following a very short charge time (the device had previously charged its capacitors, but therapy was abandoned)
EGM layout
very short charge time to deliver the shock on the T-wave (start and end of charge markers very close together)
series of 8 paced impulses at a very fast rate (200 beats/minute)
low-amplitude shock delivered on the T wave; there is a refractory period of 500 ms after shock delivery when no sensing is possible in both chambers
after the refractory period, the first ventricular event is not counted (–)
onset of a polymorphic arrhythmia with very low voltages
detection of an episode (V-Epsd) after 8 consecutive cycles in the VF zone (8/10 detection window criterion fulfilled),
first ventricular event is undersensed
after duration (1 second), detection of a sustained episode (V-Detect); start of capacitor charging
end of charge
the shock is diverted by the device (Dvrt) in the absence of reconfirmation after the end of the charge; the criterion of 2 out of 3 rapid cycles is not met; ventricular under- sensing is responsible for a false diagnosis of spontaneous arrhythmia termination
new detection window of 8 rapid cycles out of 10; start of post-detection duration
new detection of episode in VF zone (8/10 in VF zone and post-detection duration satisfied)
new, very short duration charge, the previous charge having had no time to dissipate
this shock is not reconfirmed; it is delivered following the 500 ms period at the end of charging; when a charge is diverted, the following charge for the same episode is systematically delivered due to fear of ventricular undersensing causing an incorrect diagnosis of spontaneous termination.
effective shock and arrhythmia termination
Take home message
proper defibrillator operation requires perfect sensing of the fast, low-amplitude signals of ventricular fibrillation, while simultaneously not sensing other intracardiac (non – QRS complexes) or extracardiac signals; this means programming a high sensitivity and short refractory periods; the sensitivity threshold is not programmed to a fixed value, but adapts automatically in relation to the amplitude of the preceding R wave; sensitivity then increases during the cycle, in order to search for any low-amplitude signals
Boston Scientific devices operate with a digital automatic gain control (AGC) that dynamically adjusts the sensitivity level in the atrium and ventricle; on a triple-chamber defibrillator, each channel operates with its own automatic gain control (atrial AGC, right ventricular AGC and left ventricular AGC)
before being measured, a signal is filtered according to its frequency; a bandwidth between 20 and 85 Hz is used in new-generation Boston Scientific defibrillators (the frequency of a T wave is typically between 0 and 10 Hz); a 12-bit converter converts the electrical signal into a digital value
to optimize sensing of VF signals (fast and irregular), the device adjusts ventricular sensitivity using an automatic gain control with 2 components: slow and fast
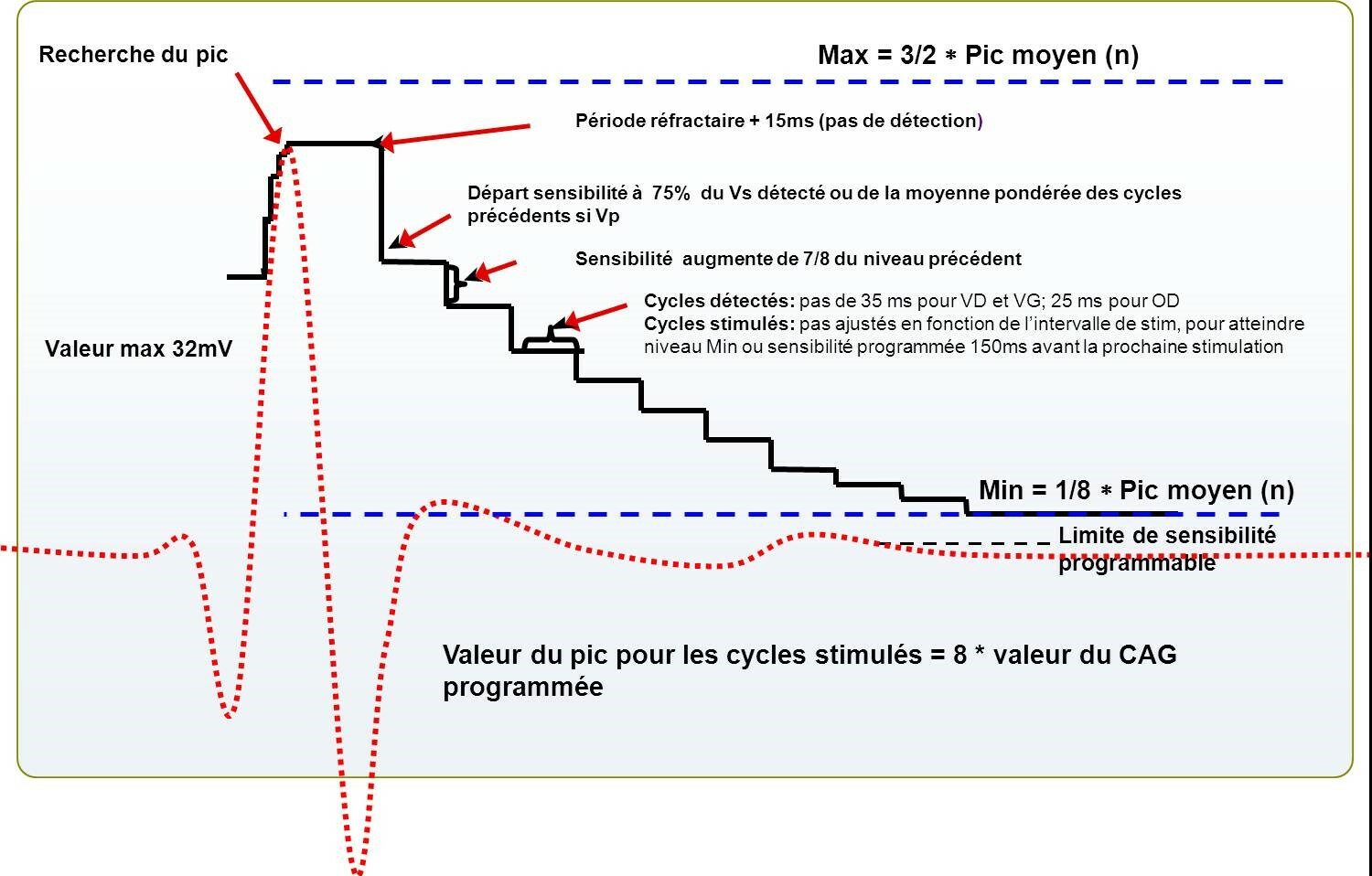
the AGC uses a so-called «slow» component to set a search interval for the amplitude of the next QRS; by calculating an «average» of the peaks of the preceding signals, the «slow» component defines a zone in which the next peak is likely to be found and sets this zone between a minimum and maximum value
after a ventricular event, the «fast» component of the AGC maintains a high sensitivity value after sensing, then decrements the sensitivity value progressively to make the device more and more sensitive; at the end of the refractory period + 15ms, the value drops to 75% of the detected peak, or 75% of the mean peak if the last ventricular event is paced; for a sensed QRS, the AGC then decreases the value to 7/8 of the previous value every 35ms; this decrease continues until the highest value between the Min or the programmed sensitivity value is reached; if the last ventricular event is paced, the AGC then decreases the value to 7/8 of the previous value at each step, but the length of the step is determined by the lower rate limit: the Min value (or the programmed sensitivity value) will be reached 150ms before the next paced event.
correct arrhythmia sensing is an essential prerequisite for shock treatment of VF; during the induction test, the maximum ventricular sensing sensitivity is usually decreased (programming of a ventricular sensitivity of 1 to 1.5 mV) so as to place the system under poor sensing conditions and increase the sensitivity of the test; good VF detection with this high value suggests a good sensing safety margin with the nominal value of 0.6 mV which will then be applied
the presentation is simple in 2 situations: 1) sensing quality is perfect throughout initial detection, duration and capacitor charging, and the safety margin in terms of sensitivity programming is deemed satisfactory; 2) sensing quality is poor, with sensing faults so frequent that the initial detection criteria are never met or the charge is systematically diverted and no therapy can be delivered; in this case, a change in lead positioning is required to obtain appropriate sensing.
sometimes, as in this patient’s case, the situation is more difficult to manage; in fact, during induction, the operator noted some ventricular sensing defects; it is important to analyze the induction tracings meticulously so as not to miss these sensing gaps, which are sometimes difficult to diagnose because they only moderately delay the onset of the shock; in this example, the first charge is diverted and the delivery of the shock is delayed by a few seconds; the graph makes it easier to identify undersensing; undersensing is favored by signal amplitude variability, which fools the automatic sensitivity control; the VF signals in this patient are highly fragmented and of low amplitude on the sensing channel, which also favors under- sensing; ventricular sensing in sinus rhythm, measured at 3.5 mV, was of average quality; despite the effectiveness of the c shock, the operator decided to move the lead from the apex of the right ventricle to the upper part of the septum, a site which enabled a very slightly higher sensing (4.4 mV in sinus rhythm).
in addition to the number of under-sensed cycles, the impact of undersensing is dependent on the detection phase; initially, 3 consecutive fast cycles are required; the detection of an episode then requires 80% fast cycles (criterion 8/10); once this criterion has been met (eliminating some oversensed episodes and extrasystoles), the device becomes a little less demanding during the initial duration and charging of the capacitors (60% rapid cycles required); at the end of charging, there is a certain «fragility» because if under-sensing occurs at this point and criterion 2/3 is not met, charging is diverted, as in this example (correct initial detection, but under-detection occurring at the end of charging).
to avoid not treating VF with under sensing, only one capacitor charge can be diverted per episode and the duration of redetection is necessarily short in the VF zone (1 second non-programmable); at the end of the duration of redetection (after a diverted charge), if a second charge begins, the shock will always be delivered (the charge cannot be diverted)
This figure shows how automatic gain control works.